Telehealth has revolutionized health care as we know it, but it may also be contributing to the overuse of antibiotics and antimicrobial resistance.
Antibiotics and the Risks
Antibiotics treat infections caused by bacteria, like strep throat and whooping cough. They do this by either killing or slowing the growth of bacteria. Antibiotics save millions of lives around the world each year, but they can also be overprescribed and overused.
Excessive antibiotic use can lead to antimicrobial resistance (AMR). AMR happens when germs from the initial infection continue to survive, even after a patient completes a course of antibiotics. In other words, the germs are now resilient against that treatment. Resistance to even one type of antibiotic can lead to serious complications and prolonged recovery, requiring additional courses of stronger medicines.
The Centers for Disease Control and Prevention reported that AMR leads to over 2.8 million infections and 35,000 deaths each year in the United States. By 2050, AMR is predicted to cause about 10 million deaths annually, resulting in a global public health crisis.
Increase in Telehealth and Antibiotic Prescriptions
Surprisingly, the growth of telehealth care may be contributing to antibiotic overprescribing and overuse.
Telehealth exploded during the COVID-19 pandemic and, today, 87 percent of physicians use it regularly. Telehealth allows patients to receive health care virtually, through telephone, video, or other forms of technology. It offers increased flexibility, decreased travel time, and less risk of spreading disease for both patients and providers.
Popular platforms like GoodRx and Doctor on Demand market convenient and easy access to health care. Others offer specialized services, like WISP that focuses on women’s health. Despite its benefits, telehealth is not perfect.
It limits physical examinations (by definition) and rapport building, which changes the patient-provider relationship. It’s also unclear whether providers can truly make accurate diagnoses in a virtual setting in some cases.
For instance, physicians were more likely to prescribe antibiotics for urinary tract infections during telehealth appointments (99%) compared to an office visit (49%). In another study, 55 percent of telehealth visits for respiratory tract infections resulted in antibiotic prescriptions, many of these cases were later found to not require them.
Glen Tullman came on THCB to talk about Transcarent’s new Wayfinding AI service. Transcarent has spent more than $125m (of the some $450m or so it’s raised so far) plugging an AI chatbot called Wayfinding into its various segments–which include the former 98.6 now rebranded as Transcarent Everyday Care. Wayfinding has benefits, clinical guidance and care delivery on one intelligent chatbot platform. No coincidence that this is released the same week as OpenAI released Chat GPT4o and the latest Google Gemini release. Make no mistake, this is a huge bet and probably the most aggressive, if obvious, use of an AI agent in health care I’ve seen so far. I saw a demo earlier which was pretty impressive and I had fun talking with Glen about what it’s capable of doing now, and what it will be–Matthew Holt
If you follow my weekly commentary on HealthCommentary.org or THCB, you may have noticed over the past 6 months that I appear to be obsessed with mAI, or Artificial Intelligence intrusion into the health sector space.
So today, let me share a secret. My deep dive has been part of a long preparation for a lecture (“AI Meets Medicine”) I will deliver this Friday, May 17, at 2:30 PM in Hartford, CT. If you are in the area, it is open to the public. You can register to attend HERE.
This image is one of 80 slides I will cover over the 90 minute presentation on a topic that is massive, revolutionary, transformational and complex. It is also a moving target, as illustrated in the final row above which I added this morning.
The addition was forced by Mira Murati, OpenAI’s chief technology officer, who announced from a perch in San Francisco yesterday that, “We are looking at the future of the interaction between ourselves and machines.”
The new application, designed for both computers and smart phones, is GPT-4o. Unlike prior members of the GPT family, which distinguished themselves by their self-learning generative capabilities and an insatiable thirst for data, this new application is not so much focused on the search space, but instead creates a “personal assistant” that is speedy and conversant in text, audio and image (“multimodal”).
OpenAI says this is “a step towards much more natural human-computer interaction,” and is capable of responding to your inquiry “with an average 320 millisecond (delay) which is similar to a human response time.” And they are fast to reinforce that this is just the beginning, stating on their website this morning “With GPT-4o, we trained a single new model end-to-end across text, vision, and audio, meaning that all inputs and outputs are processed by the same neural network. Because GPT-4o is our first model combining all of these modalities, we are still just scratching the surface of exploring what the model can do and its limitations.”
It is useful to remind that this whole AI movement, in Medicine and every other sector, is about language. And as experts in language remind us, “Language and speech in the academic world are complex fields that go beyond paleoanthropology and primatology,” requiring a working knowledge of “Phonetics, Anatomy, Acoustics and Human Development, Syntax, Lexicon, Gesture, Phonological Representations, Syllabic Organization, Speech Perception, and Neuromuscular Control.”
The notion of instantaneous, multimodal communication with machines has seemingly come of nowhere but is actually the product of nearly a century of imaginative, creative and disciplined discovery by information technologists and human speech experts, who have only recently fully converged with each other. As paleolithic archeologist, Paul Pettit, PhD, puts it, “There is now a great deal of support for the notion that symbolic creativity was part of our cognitive repertoire as we began dispersing from Africa.” That is to say, “Your multimodal computer imagery is part of a conversation begun a long time ago in ancient rock drawings.”
Throughout history, language has been a species accelerant, a secret power that has allowed us to dominate and rise quickly (for better or worse) to the position of “masters of the universe.” The shorthand: We humans have moved “From babble to concordance to inclusivity…”
GPT-4o is just the latest advance, but is notable not because it emphasizes the capacity for “self-learning” which the New York Times correctly bannered as “Exciting and Scary,” but because it is focused on speed and efficiency in the effort to now compete on even playing field with human to human language. As OpenAI states, “GPT-4o is 2x faster, half the price, and has 5x higher (traffic) rate limits compared to GPT-4.”
Practicality and usability are the words I’d chose. In the companies words, “Today, GPT-4o is much better than any existing model at understanding and discussing the images you share. For example, you can now take a picture of a menu in a different language and talk to GPT-4o to translate it, learn about the food’s history and significance, and get recommendations.”
In my lecture, I will cover a great deal of ground, as I attempt to provide historic context, relevant nomenclature and definitions of new terms, and the great potential (both good and bad) for applications in health care. As many others have said, “It’s complicated!”
But as this yesterday’s announcing in San Francisco makes clear, the human-machine interface has blurred significantly. Or as Mira Murati put it, “You want to have the experience we’re having — where we can have this very natural dialogue.”
Chakri Toleti is an occasional Bollywood film producer (you can Google that) and also the CEO of Care.ai–one of the leading companies using sensors and AI to figure out what is going on in that hospital room. They’ve grown very fast in recent years, fundamentally by using technology to monitor patients and help improve their care, improve patient safety and figure out what else is needed to improve the care process. You’ll also see me doing a little bit of self-testing!–Matthew Holt
Universities are having a hard time lately. They’re beset with protests the like of which we’ve not seen since the Vietnam War days, with animated crowds, sit-ins, violent clashes with police or counter protesters, even storming of administration buildings. Classes and commencements have been cancelled. Presidents of some leading universities seemed unable to clearly denounce antisemitism or calls for genocide when asked to do so in Congressional hearings. Protesters walked out on Jerry Seinfeld’s commencement speech; for heaven’s sake – who walks out on Jerry Seinfeld?
Derek Thompson wrote a great piece for The Atlantic that tries to pinpoint the source problem: No One Knows What Universities Are For. The sub-title sums up his thesis: “Bureaucratic bloat has siphoned power away from instructors and researchers.” As I was nodding along with most of his points, I found myself also thinking: he might as well be talking about healthcare.
Mr. Thompson starts by citing a satirical piece in The Washington Post, in which Gary Smith, an economics professor at Pomona College, argues that, based on historical trends in the growth of administration staff, the college would be best served by gradually eliminating faculty and even students. The college’s endowment could then be used just to pay the administrators.
“And just like that,” Professor Smith says, “the college would be rid of two nuisances at once. Administrators could do what administrators do — hold meetings, codify rules, debate policy, give and attend workshops, and organize social events — without having to deal with whiny students and grumpy professors.”
It’s humorous, and yet it’s not.
The growth in universities’ administrative staff is widespread. Mr. Thompson acknowledges: “As the modern college has become more complex and multifarious, there are simply more jobs to do.” But that’s not always helping universities’ missions. Political scientist Benjamin Ginsberg, who published The Fall of the Faculty: The Rise of the All-Administrative University and Why It Matters in 2014, told Mr. Thompson: “I often ask myself, What do these people actually do? I think they spend much of their day living in an alternate universe called Meeting World.”
Similarly, Professor Smith told Mr., Thompson it’s all about empire building; as Mr. Thompson describes it: “Administrators are emotionally and financially rewarded if they can hire more people beneath them, and those administrators, in time, will want to increase their own status by hiring more people underneath them. Before long, a human pyramid of bureaucrats has formed to take on jobs of dubious utility.”
All of these administrators add to the well-known problem of runaway college tuition inflation, but a more pernicious problem Mr. Thompson points to is that “it siphons power away from instructors and researchers at institutions that are—theoretically—dedicated to instruction and research.”
The result, Mr. Thompson concludes is “goal ambiguity.” Gabriel Rossman, a sociologist at UCLA, told him: “The modern university now has so many different jobs to do that it can be hard to tell what its priorities are.” Mr. Thompson worries: “Any institution that finds itself promoting a thousand priorities at once may find it difficult to promote any one of them effectively. In a crisis, goal ambiguity may look like fecklessness or hypocrisy.”
So it is with healthcare.
Anyone who follows healthcare has seen some version of the chart that shows the growth in the number of administrators versus the number of physicians over the last 50 years; the former has skyrocketed, the latter has plodded along. One can – and I have in other forums – quibble over who is being counted as “administrators” in these charts, but the undeniable fact is that there are a huge number of people working in healthcare whose job isn’t, you know, to help patients.
It’s well documented that the U.S. healthcare system is by far the world’s most expensive healthcare system, and that we have, again by far, the highest percent spent on administrative expenses. Just as all the college administrators helps keep driving up college tuition, so do all those healthcare administrators keep healthcare spending high.
But, as Mr. Thompson worries about with universities, the bigger problem in healthcare is goal ambiguity.
Given that I ran a health technology conference for many years, I tend to run in a circle of people who have some ambition to get rich in health care. After all, billions of dollars of VC money have been dropped in lots of startups over the last decade, and a few prime examples have done very well. For example Jeff Tangey of Doximity, Glen Tullman of Livongo, Chaim Indig of Phressia and many others did fine when their companies IPOed in the late 2010s. But the truth is that many, many more have either started a health tech business that didn’t make it, or were foot soldiers in others that died along the way (Olive, Babylon, Pear, etc, etc). Which has been leading me lately to thinking about whether that’s the right approach to take if you want to make money in health care. Hint: it’s not.
There’s still tremendously little transparency about which health care organizations have what amount of money and what people earn. There is though one sector that by law has to publish information about revenue, profits, investments and executive compensation. That is the non-profit hospital/health system sector. Nonprofits are required to file Form 990 with the IRS that has that information and more on it. Having said that, most hospitals are frequently late in filing them, and file them in a very confusing way. The wonderful journalism organization ProPublica maintains a database of all 990 filings and it’s instructive to look around in it.
Some health systems make it relatively easy. UPMC, the huge western PA conglomerate files one 990 for the whole group. Others, not so much. I know that Providence, the huge west coast system, has overall revenue of $28bn but only because Fierce Healthcare told me. Had I tried to piece that together from its 990s, I’d have started with its Washington filing ($6bn), moved on to its Oregon filing (~$5bn) and then started getting confused..
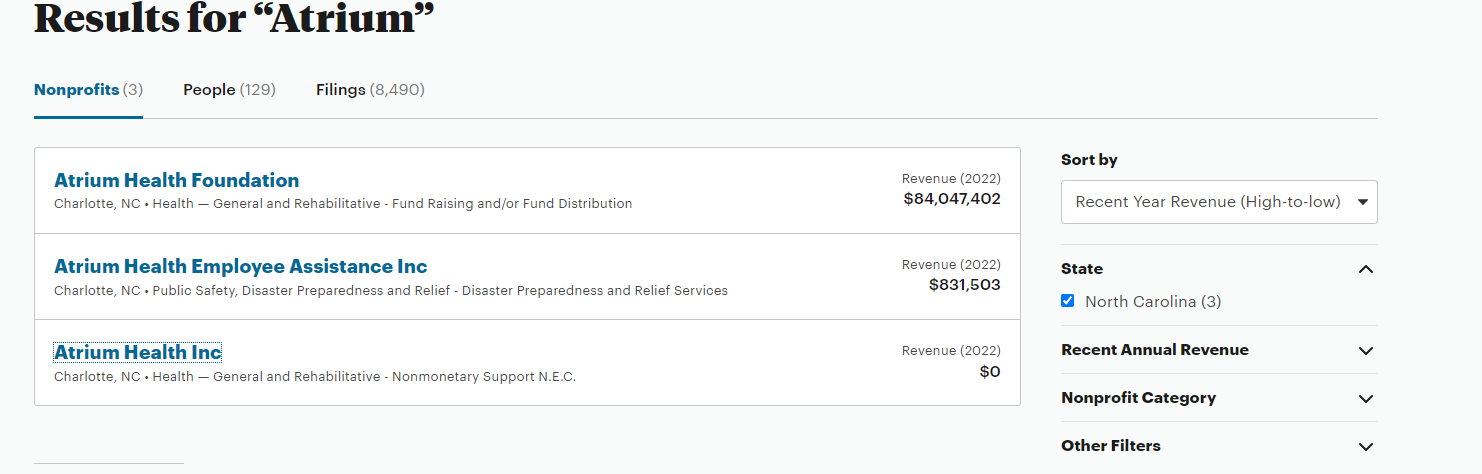
Let’s say you wanted to easily figure out Advocate, the system that was the merger of the huge midwestern system with Atrium, the North Carolina-based one. Good luck. You can find Advocate but Atrium’s seems to be missing. Ditto for Carolinas Health, its previous name. There is a page calling itself Financial Information on the Atrium website, but it doesn’t have any, and tells you to go to a website set up for municipal bondholders. In fact I couldn’t find any evidence of the IRS auditing any large system, or fining them for non-compliance in filing.
The good news is that last year the North Carolina State Employees plan, i.e. a pissed off purchaser, dug into all the N. Carolina hospital systems and found out that Atrium’s CEO pay went up nearly five-fold over six years. But even the state had real trouble finding out the truth:
“It is important to understand that these figures are significant underestimates for three reasons. First, a legal loophole denies the public the right to see how much publicly owned hospitals reported paying their top executives on their tax filings. This failure of oversight hides the tax filings of more than three in 10 nonprofit hospitals in North Carolina, including Atrium and UNC Health. UNC Health did not answer a public records request for executive compensation data until February 13, 2023, two days before this report’s publication and almost three months after its receipt of the request. UNC Health’s system wide data is therefore not included in this report.”
So the very top dogs are doing well. At UPMC it turns out that seven made more than $3m including the CEO Jeff Romoff –the same one who forgot on 60 Minutes whether he made $6m or $7m. Turns out he didn’t have to remember that number for long as by 2021 he was making $12m.
But the munificence is spreading down the executive ladder. To demonstrate, let me introduce you to Tracey Beiriger Esq. There’s almost no information about Tracey on Linkedin or anywhere else on Google other than it appears he or she is an IP lawyer at UPMC. So why do I bring them up?
Because in 2021–the last year for which UPMC filed a 990 –Tracey was the 118th highest paid executive at UPMC and had the misfortune to only make $499,446.
Which means that 117 executives working at UPMC made more than $500,000. It’s a little tricky figuring out the similar numbers at Providence because of the multiple 990s in 2021 but there are 38 in Washington (not including CEO Rod Hochman who made $9m in 2020 and then vanished from the 2021 990!), 18 in Oregon and another 21 in Southern California. So call it 80+.
I bring this up because $500,000 is a pretty decent individual income. When I asked ChatGPT it estimated about 1.2 million Americans earned that much or more. Given the workforce is 167m, that puts those several hundred hospital execs way into the top 1%.
Now I have no objection to people earning good money. I’m sure they have all worked very hard for it. But if you look at these organizations, they do not seem to be spreading the wealth very far.
Last year UPMC was accused by unions of suppressing staff wages. There is yet to be an outcome from that complaint to the DOJ, but last week there was one from a formal class action complaint about Providence shortchanging employees by rounding down their pay to the nearest half-hour, even though they were clocking on and off by the minute. Providence was fined $200m which probably isn’t much split between 33,000 employees but at least indicates that their senior management acts just like any other aggressive business in terms of cutting costs on the backs of their employees. And it’s not just their employees. They also just got fined $137m for aggressively suing patients.
Which leads me to two final points.
The first is, is it more likely you’ll make that $500K+ in a hospital system or in a tech startup? Blake Madden at Hospitology has been tracking systems that have more than $1bn in revenue. He’s found 113 so far. Second bottom of the list is Atlanticare in NJ, which has 16 execs making more than $500K. Which by my wild guess means that the average system has about 50 employees making $500k+ which rounds up to something like 5,000 hospital execs making at least $500K and many of them are making a whole lot more.
Compare that to a successful health tech startup that actually makes it. Take Phreesia, a VC-backed start-up that went public in 2019 having started way back in 2007. (I know the year because CEO Chaim Indig launched at Health 2.0 in 2008. He was nice enough to let me buy some stock at the IPO and I made a few bucks). Chaim made $300K the year it went public and as CEO of a public company that’s bounced around at being worth between $1Bn and $4Bn, he made $750K last year. No one else made more than $500K. Now yes, he owned 4% of the company at the IPO and got awarded more stock. He is doing very well, but the point is that there were dozens of companies launching at Health 2.0 in 2008 and the vast majority don’t get close to an IPO or making any money for the founders, let alone the staff.
My conclusion is, it’s not a rational bet to go the health tech route if instead you can find a regional hospital chain and brown-nose your way up into the exec ranks!
The second point is more fundamental. Remember UPMC and its 117 execs making $500K+? What would a comparable government agency be paying out? I looked at the state of California salaries.There look to be about 50 state employees making more than $500k a year, almost all working for the state investment fund CALPERS. But the top paying one only makes $1.6m a year. I’m not saying that CALPERS should be paying out that much even if it is competing with Wall Street, after all members of the Senate only make $205,000 a year and the state could just put the whole pension into an S&P index fund. But what I am saying is that we should be thinking about paying our big non-profit systems similarly to government employees because they essentially are government employees.
Beckers posted UPMC’s payor mix last year. I highly suspect you’ll find something similar at almost every big system.
Medicare 48%
Medicaid 17%
UPMC as Insurer 11%–(60% of whom are Medicaid/Medicare patients)
Commercial, Self Pay, Other 24%
More than 70% of the money comes from the government, and the rest from the suckers who have to buy their insurance on the “open market”–which includes those buying via the ACA exchange, receiving government subsidies, and government employees.
So while these huge systems act like Fortune 100 companies and reward their executives accordingly, almost all the money comes from the taxpayer.
I wish I could say we are getting good value for it.
And yes, I didn’t even mention the for-profits and the big insurers, but that will have to wait for another day….
America is crazy about gambling. Once you had to gamble illegally with a bookie, or go to Atlantic City or Las Vegas; now 45 states – plus the District of Columbia, Puerto Rico, and the U.S. Virgin Islands – have state lotteries. Since the Supreme Court struck down PASPA, the federal ban on sports betting, 38 states – plus the D.C. and Puerto Rico – offer legal sports betting. I didn’t think we could get any crazier, until I saw last week that arcade chain Dave & Busters was going to allow betting on some of its games.
Honestly, healthcare may be the only industry upon which you can’t bet, and I’m beginning to think that’s too bad.
Dave & Busters are working with Lucra Sports, a “white-label gamification” technology company. “We’re thrilled to work with Lucra to bring this exciting new gaming platform to our customers,” said Simon Murray, SVP of Entertainment and Attractions at Dave and Buster’s. “This new partnership gives our loyalty members real-time, unrivaled gaming experiences, and reinforces our commitment to continuing to elevate our customer experience through innovative, cutting-edge technology.”
“Friendly competition really is a big fuel for our economy, whether you’re playing golf on Sunday with your buddies, or you’re going to play pickleball or video games or even cornhole at a tailgate. There’s so many ways that you can compete with friends and family, and I think gamifying that and digitizing all this offline stuff that’s happening is a massive opportunity,” Lucra CEO Dylan Robbins told CNN.
The companies are careful not to describe what they’re doing as gambling; they avoid terms like “bet” or “wager.” Michael Madding, Lucra’s chief operating officer, told The New York Times that the focus was on “skills-based” games, such as Skee-Ball or shooting baskets: i.e., “recreational activities for which the outcome is largely or entirely dependent on the knowledge, ability, strength, speed, endurance, intelligence of the participants and is subject to the control of those participants.”
This falls into a category I had never heard of: “social betting.” With social betting, there is no third party setting the odds, and more head-to-head competition with people you know. You’re not betting against the house; you’re challenging your friends. It is estimated by gaming research firm Eilers & Krejcik to be a $6b market, and its proponents argue that it is not subject to licenses & regulations that other gambling does.
Not everyone agrees. Marc Edelman, a law professor and the director of sports ethics at Baruch College in New York, told NYT:
If two people are competing against one another in Skee-Ball, presuming that there is nothing unusual done in the Skee-Ball game and physical skill is actually going to determine the winner, there is no problem. If I am taking a bet on whether someone else will win a Skee-Ball game, or whether someone else will achieve a particular score in Skee-Ball, if I myself am not engaged in a physical competition, that very likely would be seen as gambling.
Brett Abarbanel, executive director of the University of Nevada, Las Vegas, International Gaming Institute, went further, telling CNBC: “regardless of the legal classification of the activity as ‘not gambling’ vs. ‘gambling,’ this is an activity in which participants are risking something of value on an outcome that is uncertain. Therefore, there should be consumer protection measures in place for players, particularly when the target audience is skewed toward younger participants.”
Both Illinois and Ohio gambling authorities have already expressed concerns; Illinois State Rep. Daniel Didech, chairman of the Illinois House Gaming Committee,, told CNBC: “It is inappropriate for family-friendly arcades to facilitate unregulated gambling on their premises. These businesses simply do not have the ability to oversee gambling activity in a safe and responsible manner.”
There are also numerous “social sportsbooks,” including Flitt, PrizePicks, and Underdog Fantasy, that are blurring the line between online sports gambling and social betting, between fantasy leagues and plain old gambling. And they do it with users as young as 13 and with little or no state oversight. Keith Whyte, executive director of the National Council on Problem Gambling, told The Washington Post: “What a lot of these social gaming — social casinos, social sportsbooks — have found is that the regulators … either don’t feel like they have the jurisdiction or the time or energy to go after every single app that springs up.”
Whether we like it or not, people are going to bet. “People will place a bet on ‘Will we have rainfall?’, or ‘How much snow will a certain place get?’, or ‘What will be the first day of snowfall?’” sports policy expert John Holden, JD/PhD, associate professor at Oklahoma State University, told Fox 5 NY last year.
If you talk to consultants about AI in Medicine, it’s full speed ahead. GenAI assistants, “upskilling” the work force, reshaping customer service, new roles supported by reallocation of budgets, and always with one eye on “the dark side.”
But one area that has been relatively silent is surgery. What’s happening there? In June, 2023, the American College of Surgeons (ACS) weighed in with a report that largely stated the obvious. They wrote, “The daily barrage of news stories about artificial intelligence (AI) shows that this disruptive technology is here to stay and on the verge of revolutionizing surgical care.”
Their summary self-analysis was cautious, stating: “By highlighting tools, monitoring operations, and sending alerts, AI-based surgical systems can map out an approach to each patient’s surgical needs and guide and streamline surgical procedures. AI is particularly effective in laparoscopic and robotic surgery, where a video screen can display information or guidance from AI during the operation.”
The automatic emergency C-Section in Prometheus–Coming, but not quite yet!
So the ACS is not anticipating an invasion of robots. In many ways, this is understandable. The operating theater does not reward hyperbole or flash performances. In an environment where risk is palpable, and simple tremors at the wrong time, and in the wrong place, can be deadly, surgical players are well-rehearsed and trained to remain calm, conservative, and alert members of the “surgical team.”
Demand for GLP-1 medications soared last year and shows no signs of stopping in 2024. Employers and health plans are understandably anxious about how long they should expect to pay for these pricey drugs. They’re itching for an easy off-ramp.
Some solutions are cropping up to pave the way. Many of them claim they can help patients reap the benefits of GLP-1s within a short time frame, and get them off the drugs within 12 months to save costs. But the data doesn’t support that promise. In fact, studies suggest some patients may need to stay on the drugs indefinitely to sustain outcomes while other patients may be able to discontinue the drugs and at least maintain their cardiometabolic risk reduction even if they cannot maintain all of their weight loss.
A better strategy to control costs is to more accurately pinpoint those who really need the drugs—and keep those who don’t off of them from the start. Of course, there will be times when deprescribing is appropriate, and we need to clinically support patients through that process. But one-size-fits-all solutions centered on medication as a silver bullet to obesity are only setting up patients and payers for failure. Similarly, those whose sole promise is to deprescribe, don’t follow the evidence.
Prescribing GLP-1s with the goal to deprescribe is foolhardy
GLP-1s treat obesity, but they don’t cure it. GLP-1 agonists increase the body’s own insulin production and slow the movement of food from the stomach to the small intestine. The drugs help people eat less by curbing cravings and boosting satiety. Studies show that once people go off semaglutide, the cravings come back in full force—and so does much of the weight.
While GLP-1 medications produce nearly miraculous outcomes in some people, they’re no quick fix. Obesity is a complex chronic disease. Drugs alone can’t solve for genetic predisposition, behaviors, mental and emotional components, social determinants of health, and other compounding elements that contribute to obesity. In the right circumstances, drugs can give people a solid leg up in better managing those contributing factors—but they’re not for everyone.
Keto is not a sustainable replacement for GLP-1s
Highly restrictive diets like the keto diet aren’t for everyone either. Keto requires a drastic reduction in carbohydrate intake, which can be difficult to maintain long-term. Not to mention, the high-fat content of keto diets can also lead to other health issues and isn’t conducive to tapering off of GLP-1 medications. Side effects from the drugs can make a high-fat diet difficult to tolerate.
It’s good to be wary of solutions that promise an off-ramp by way of highly restrictive diets. While a keto diet may help people lose weight in the short term, studies show that weight loss is rarely sustained over the long run and may be detrimental to overhaul health. The diet is associated with many complications that often lead to hospital admissions for dehydration, electrolyte disturbances, and hypoglycemia.
Triage the right care to the right people at the right time
Obesity’s complex nature requires a personalized approach to treatment that delivers the right care to the right people at the right time. That takes a whole care team of specialized providers—like registered dietitians, health coaches, and prescribing physicians to help people at various stages of the disease. And since obesity often occurs alongside other cardiometabolic conditions like hypertension, diabetes, COPD, and more, patients need the help of specialists who understand how those different conditions interact.
Soon after Apple released the original iPhone, my father, an unlikely early adopter, purchased one. His plan? “I’ll keep it in the trunk for emergencies,” he told me. He couldn’t foresee that this device would eventually replace maps, radar detectors, traffic reports on AM radio, CD players, and even coin-operated parking meters—not to mention the entire taxi industry.
His was a typical response to revolutionary technology. We view innovations through the lens of what already exists, fitting the new into the familiar context of the old.
Generative AI is on a similar trajectory.
As I planned the release of my new book in early April, “ChatGPT, MD: How AI-Empowered Patients & Doctors Can Take Back Control of American Medicine,” I delved into the promise and perils of generative AI in medicine. Initially, I feared my optimism about AI’s potential might be too ambitious. I envisioned tools like ChatGPT transforming into hubs of medical expertise within five years. However, by the time the book hit the shelves, it was clear that these changes were unfolding even more quickly than I had anticipated.
Three weeks before “ChatGPT, MD” became number one on Amazon’s “Best New Books” list, Nvidia stunned the tech and healthcare industries with a flurry of headline-grabbing announcements at its 2024 GTC AI conference. Most notably, Nvidia announced a collaboration with Hippocratic AI to develop generative AI “agents,” purported to outperform human nurses in various tasks at a significantly lower cost.
According to company-released data, the AI bots are 16% better than nurses at identifying a medication’s impact on lab values; 24% more accurate detecting toxic dosages of over-the-counter drugs, and 43% better at identifying condition-specific negative interactions from OTC meds. All that at $9 an hour compared to the $39.05 median hourly pay for U.S. nurses.
Although I don’t believe this technology will replace dedicated, skilled, and empathetic RNs, it will assist and support their work by identifying when problems unexpectedly arise. And for patients at home who today can’t obtain information, expertise and assistance for medical concerns, these AI nurse-bots will help. Although not yet available, they will be designed to make new diagnoses, manage chronic disease, and give patients a detailed but clear explanation of clinician’ advice.
These rapid developments suggest we are on the cusp of technology revolution, one that could reach global ubiquity far faster than the iPhone. Here are three major implications for patients and medical practitioners:
1. GenAI In Healthcare Is Coming Faster Than You Can Imagine
The human brain can easily predict the rate of arithmetic growth (whereby numbers increase at a constant rate: 1, 2, 3, 4). And it does reasonably well at comprehending geometric growth (a pattern that increases at a constant ratio: 1, 3, 9, 27), as well.
But even the most astute minds struggle to grasp the implications of continuous, exponential growth. And that’s what we’re witnessing with generative AI.