OpenAI just made ChatGPT Health generally available. This is their partnership with B.Well which allows you to bring your data from various EMRs into chatGPT. So I took it for a spin–Matthew Holt
Future of AI and Telehealth in primary care — Panel discussion
A couple of months back I hosted a conversation about my favorite topics, primary care and how telehealth and AI are changing it. The panel was Timm Schneider — Co-Founder & COO, Third Way Health, Jamie Reddick — COO, Graybill Medical Group & Erin Parks, Ph.D. — Co-Founder, Equip. The panel was at a tech heavy conference called TechCon Global in San Diego. Sadly the weather stopped us getting Matt Siegler from Akido Labs. We got into it about tech. incentives, specialty care and the role of AI in access and patient support–Matthew Holt
A ridiculously stupid letter from a health insurer

By MATTHEW HOLT
It’s hard to imagine but I may now be in possession of the stupidest letter I’ve ever received from an American health insurance company–-and I’m the guy who got five identical letters on one day from Blue Shield of California telling me that they had changed my primary care doctor when I had initiated the change.
A little backstory. As those you’ve been following along with my various telenovelas may remember that last year I was diagnosed with a failing heart valve. I also have a failing left knee due mostly to snowboarding into a tree 24 years ago.
I was attempting to put off doing anything about the heart valve for as long as possible because it sounds painful and unpleasant, and I was hoping that I could go ahead with a knee replacement so that my snowboarding can continue apace. My doctors are at UC San Francisco and they agreed that I should have the knee replacement on July 6th, assuming that my heart valve had not got much worse. On June 16th I went into UCSF for a bunch of knee replacement pre-workup and they also checked my heart.
However, my new insurance company, thanks to my wife’s new job, is Cigna. Those of you in California may know that Cigna was having a big dispute with the University of California Health system and that its contract with them was due to expire on June the 30th of this year. Why a health plan and a big provider organization have contracts that expire in the middle of the year when the employers and people who use the health plan network buy them on an annual basis starting in January I don’t know – and it’s ridiculously stupid. But let’s not get distracted cause I’m not talking about that here!
Because of the fact that they’d be out of network, the ortho team made the obvious suggestion that I move the knee replacement a little earlier, In fact it was planned for June the 22nd. This did not upset me too much as you may have seen that some corrupt Italians have organized a soccer tournament that would give me plenty of games on TV to be entertained by while I was lying around recovering.
Sadly one of the pretests I had on June 16th was an echocardiogram that indicated that my heart valve was in even worse shape than it had been earlier in the year. After quite a lot of back and forth between the cardiac team, the knee team and the anesthesia team, everyone agreed to put off the knee surgery until we figured out my heart.
Meanwhile sometime late on Thursday the 25th or early on Friday the 26th of June, UC Health and Cigna stepped back from the brink and came to an agreement that will continue the UC system being in Cigna’s network.
Which all brings me to July 6th when I received a letter from Cigna
This is the one that contains more stupidity per square inch than any other communication I’ve had from an insurance company.
Continue reading…THCB Spotlight: Warris Bokhari, Claimable
One of the most interesting follows on Linkedin is Warris Bokhari from Claimable. He’s a British MD, who has had stints not only as a doc in the UK, but also as a health tech and health insurance exec in the US. But now he’s at war with the system, in particular working for patients to overturn denials from insurers using AI. But what exactly is the big picture aim, and how does Warris think that he’s going to fix American health care? We had quite the discussion and we sort of agree, but also don’t. Great discussion and transcript is below the video–Matthew Holt
This was such a great discussion I wanted to publish the transcript. The way I do that is to copy the Youtube generated transcript and drop it into Claude to smooth it over. I then read it and if I think it’s made an error, dip back into the video and listen to what actually happened and make a correction. This is all code therefore for me saying I think this transcript is pretty accurate but it might have a bunch of AI and human generated mistakes.
THCB Spotlight: Warris Bokhari, CEO of Claimable
Continue reading…Ellipsis Health
Ellipsis Health has come a long way from its roots in detecting depression via vocal biomarkers. Sage, its charming voice AI agent, is now helping health plans and care management companies directly interact with patients and members, helping them with medication reminders, program recruitment, postop follow up and much more. I spoke with two of the brains behind Sage, COO Melissa McCool and CMO Mike Aratow. We got into what she does, what she’s good at and whether the world (or at least the health care world) needs specific voice AI specialists–Matthew Holt
Schrodinger’s Co-pay
By MATTHEW HOLT
More tales of the woes of dealing with health insurance. I live in Marin County, California and one of the things that comes with that is a diagnosis of ADHD for my children. (OK, I have made that joke before but it is true!). My kids now visit a psychiatrist for more sophisticated med management than they receive at their pediatrician. We were (until recently) on a Blue Shield HMO via the Covered California exchange.
While I was at the doctor’s office, I talked to the staff. They told me I owed a $50 copay. I didn’t pay them (yet) and I went online and saw the claim
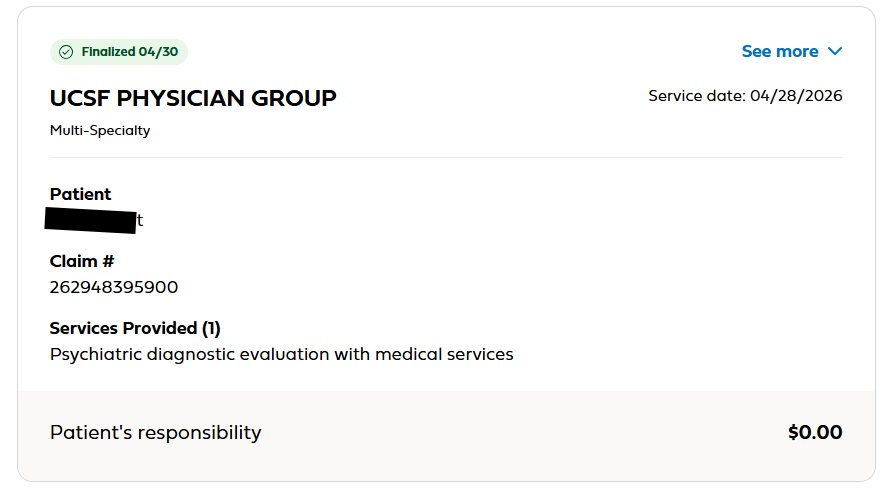
The reasonable, informed consumer might think that I owed nothing. The clue being that
“Patient Responsibility” was $0.
But if you click the “See More” in the top right it shows you this
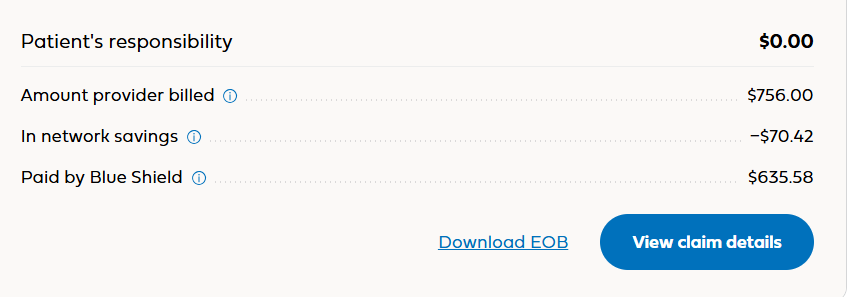
You probably still think that I owe $0. But if you add the numbers on the right you might notice they don’t total $0.
Continue reading…Dor Skuler, Intuition Robotics: Meet ElliQ
Dor Skuler is CEO of Intuition Robotics the maker of ElliQ — a remarkable AI robot that is a companion for seniors. I had a lot of fun meeting ElliQ and asking Dor about how she works. This is a wide-ranging interview with Dor and with ElliQ. She tells us about Florence Nightingale, what Dor should do with his kids and really gives you the idea of how she relates to seniors. There’s a ton of capabilities–you really have to watch the whole thing–but the end result is that Medicaid plans including NY and Washington State have determined that ElliQ allows people to stay at home longer and saves $$ on nursing home care. A fascinating view into the present and the future of how AI and robotics is changing the world–Matthew Holt
New Podcast on Primary Care
This is one of those “Coming Soon” announcements. I spent the weekend with the wonderful gang from what I affectionately call Camp Claudia Cult, a group of mostly Californian policy wonks led by Claudia Williams, who these days is at the UC Berkeley School of public health. As you may have noticed I’ve been spending much of my time writing and talking about the notion of Concierge Care for All. Most of the group at the Health Collab wants to blow up/burn down the current system and replace it with a primary care-driven system. And there’s lots of discussion and planning on how to do that. But there is so much happening in innovation in primary care that I thought we need a dedicated channel to discuss it.
Since the sunsetting of the THCB gang, I’ve been doing lots of tech interviews, but not many about how care works. So now I will. If you want to get involved or be interviewed, please email me — Matthew Holt
Ben Salter, SafeRide Health
Ben Salter is the Chief Product Officer of SafeRide Health. They are one of the biggest players in non-emergency medical transport (NEMT) working predominantly for health plans that have Medicaid or Medicare Advantage members. Getting people to their appointments is a big deal–think disabled or sick people who will miss clinical appointments if they can’t get there. Ben showed a demo of how their system works, what it looks like for call center staff or members using it directly, and how that then actually gets someone a ride to where they need to go–Matthew Holt
Bribery, Corruption and the American Health Care Way
By MATTHEW HOLT
These days you just have to wonder about the greed and corruption that is going on all around. Senator Dick Blumenthal is one of many who’ve been pointing out the naked corruption in the Trump family–Qatari jets, memecoins, Trump’s son being on the board of so many defense and prediction market companies you can’t keep it straight. Issac Saul has tried to detail it all, but reading just the cryptocurrency part of his piece has me spinning. And we’re nowhere near assessing the naked corruption of so many others in the administration. Kristi Noem, despite being fired, is still living in her government house, and has not had to answer for routing some of a totally unnecessary $220m ad campaign to a company that her friends own. The company was incidentally established a whole 8 days before it got the contract.
So it’s a little absurd to be worrying about fraud and corruption in health care. But apparently HHS is. At least Oz and RFK Jr are going on about Somalis defrauding Medicaid and Armenians running fake hospices in California. (Let’s not even consider the optics of a Turkish citizen with close ties to the Erdogan regime criticizing Armenians–I mean the genocide was over a century ago!)
But of course, fraud and corruption in health care has been going on forever. Back in 2011 a Florida man was convicted of Medicare fraud to the tune of tens of millions and got a 50 year sentence. Don’t be surprised that Trump commuted his sentence. And that’s just one of thousands and thousands of cases, mostly by providers inventing fake patients to defraud Medicare or Medicaid.
But the ones who get convicted and go to jail are the amateurs.
If you’re a big company in health care, you fight with lawyers and you settle. For example, every big pharma company has settled for things like off-label promotion of their drugs. GSK paid $3bn, Pfizer over $2bn, J&J over $2bn. In fact back in the 2000s THCB had a regular correspondent called The Industry Veteran who basically suggested that whistleblowing in qui tam suits inside big pharma was the way to wealth and fame. And of course HCA in its days when it was run by Rick Scott – now (somehow not a) convicted felon as well as Florida senator – settled for $1.7bn. This was all back in the 1990s and early 2000s, but it’s all still going on.
The venue though may have moved. Risk adjustment in Medicare Advantage has become one of the biggest venues for fraud. The key here is that the DOJ and HHS found that while Medicare Advantage plans were upcoding their patients, and therefore getting paid more for them, they weren’t actually delivering more services.
Continue reading…






