A couple of months back I hosted a conversation about my favorite topics, primary care and how telehealth and AI are changing it. The panel was Timm Schneider — Co-Founder & COO, Third Way Health, Jamie Reddick — COO, Graybill Medical Group & Erin Parks, Ph.D. — Co-Founder, Equip. The panel was at a tech heavy conference called TechCon Global in San Diego. Sadly the weather stopped us getting Matt Siegler from Akido Labs. We got into it about tech. incentives, specialty care and the role of AI in access and patient support–Matthew Holt
How Online Prescription Services Are Closing the Access Gap for Patients Who Skip the Doctor’s Office

By DAMIAN WONJO
Every clinician keeps a private list of the patients they don’t see. Not the ones who cancel, the ones who never book. The shift worker who reschedules the same appointment three times and then quietly gives up. The parent who can’t justify half a day off and a waiting-room afternoon for a routine refill. The patient whose condition carries enough stigma that the friction of a face-to-face visit becomes, in itself, a reason to do nothing. These people don’t show up in no-show statistics. They show up later, as complications, as emergencies, as avoidable deterioration.
This is the access gap, and from where I sit as a physician in Europe, it has less to do with the raw supply of doctors than with the cost of reaching one, measured not only in money but in time, distance, and effort. When that cost climbs higher than a patient’s tolerance, care simply doesn’t happen. Online prescription services and remote consultation won’t fix every part of this problem. But they target precisely the variable that most reforms ignore, which is friction.
The patients who fall through
It is tempting to frame telemedicine as a convenience for the already-healthy and already-connected. In practice, the people who benefit most are often those with the least slack in their lives. A patient stabilised on the same antihypertensive for three years does not need a fresh diagnostic odyssey to continue it, they need a prescription before they run out. A working adult who recognises a recurring, familiar problem does not always need a physical examination to be helped safely. Forcing every such encounter through the narrow door of an in-person appointment does not raise the standard of care, it raises the rate at which people abandon it.
Continuity is where this matters most. Chronic conditions are managed in refills, and a missed refill is not a clerical event but a gap in treatment with real physiological consequences. Lowering the barrier to that refill is not a luxury. It is, quietly, one of the highest-yield interventions available.
What changed in Europe
The pandemic did not invent telemedicine, but it normalised it, and it accelerated the infrastructure underneath it. Poland is a useful case study. Electronic prescriptions became the national standard in 2020, and today essentially every prescription is issued digitally, retrievable by the patient through a government health account and dispensable at any pharmacy with a code. The clinical encounter and the prescription were decoupled from a single physical location without being decoupled from a licensed prescriber.
That distinction is the whole argument. A responsible online prescription service is not a vending machine. It is a licensed physician, working within the same legal and ethical framework as any clinic, using a different channel to reach the patient. The technology is mundane. The consequence, that a patient who would otherwise have gone without is now seen, is not.
Continue reading…A ridiculously stupid letter from a health insurer

By MATTHEW HOLT
It’s hard to imagine but I may now be in possession of the stupidest letter I’ve ever received from an American health insurance company–-and I’m the guy who got five identical letters on one day from Blue Shield of California telling me that they had changed my primary care doctor when I had initiated the change.
A little backstory. As those you’ve been following along with my various telenovelas may remember that last year I was diagnosed with a failing heart valve. I also have a failing left knee due mostly to snowboarding into a tree 24 years ago.
I was attempting to put off doing anything about the heart valve for as long as possible because it sounds painful and unpleasant, and I was hoping that I could go ahead with a knee replacement so that my snowboarding can continue apace. My doctors are at UC San Francisco and they agreed that I should have the knee replacement on July 6th, assuming that my heart valve had not got much worse. On June 16th I went into UCSF for a bunch of knee replacement pre-workup and they also checked my heart.
However, my new insurance company, thanks to my wife’s new job, is Cigna. Those of you in California may know that Cigna was having a big dispute with the University of California Health system and that its contract with them was due to expire on June the 30th of this year. Why a health plan and a big provider organization have contracts that expire in the middle of the year when the employers and people who use the health plan network buy them on an annual basis starting in January I don’t know – and it’s ridiculously stupid. But let’s not get distracted cause I’m not talking about that here!
Because of the fact that they’d be out of network, the ortho team made the obvious suggestion that I move the knee replacement a little earlier, In fact it was planned for June the 22nd. This did not upset me too much as you may have seen that some corrupt Italians have organized a soccer tournament that would give me plenty of games on TV to be entertained by while I was lying around recovering.
Sadly one of the pretests I had on June 16th was an echocardiogram that indicated that my heart valve was in even worse shape than it had been earlier in the year. After quite a lot of back and forth between the cardiac team, the knee team and the anesthesia team, everyone agreed to put off the knee surgery until we figured out my heart.
Meanwhile sometime late on Thursday the 25th or early on Friday the 26th of June, UC Health and Cigna stepped back from the brink and came to an agreement that will continue the UC system being in Cigna’s network.
Which all brings me to July 6th when I received a letter from Cigna
This is the one that contains more stupidity per square inch than any other communication I’ve had from an insurance company.
Continue reading…Life Not As We Know It

By KIM BELLARD
Well, let’s see. Last week much of the U.S. and parts of Europe were under a crippling heat dome. The U.S. celebrated its 250th birthday. And there’s something called the World Cup going on, for those of you who care about such things. But, I mean, really, the news of the week? SpudCell.
OK, maybe you missed that one. If you are not a fan of science, or of synthetic biology in particular, news about it might not have shown up in your feeds, or perhaps you thought it was another ploy by the Potato Association of America to get you to buy even more potatoes. SpudCell is something truly new: “the world’s first synthetic cell with a complete life cycle, built entirely from non-living chemical components.”
Take a minute to take that description in.
“SpudCell performs the behaviors often used to tell the living from the inert — it feeds, grows, replicates its genome, divides and undergoes selection — yet it is far simpler than any natural cell and was assembled, part by part, by hand,” the project researchers wrote in a statement.
It was designed and built by researchers at the University of Minnesota, announced last week along with a preprint of their paper.The team was led by Professor Kate Adamala, and the name is either due to its supposed resemblance to a potato or it’s a play on “Sputnik.”
“This is likely the most exciting project I’ve ever worked on,” said Professor Adamala. “We’ve replicated in chemistry what only used to be possible in biology: the complete set of behaviors of a cell. It proves that the most fundamental functions of life, like growth and replication, do not need a mysterious magical spark.”
Scientists have been working for decades on stripping away genetic material from living cells to try to find the minimum necessary for life, but Professor Adamala and her team went the other way, gradually building up genetic material until it started behaving in ways we’d expect cells to.
The impressive thing is that the team engineered everything SpudCell does. As The Economist put it: “Everything the resulting cells do, they do because of molecules that Dr Adamala’s team put there. That leaves no room for mysteries.” That’s not true when researchers start with living cells.
Drew Endy, a synthetic biologist at Stanford University, told Carl Zimmer of The New York Times, “It’s a cell that was built, not born. It’s constructed, but it does what cells do.”
SpudCell is very basic.
Continue reading…THCB Spotlight: Warris Bokhari, Claimable
One of the most interesting follows on Linkedin is Warris Bokhari from Claimable. He’s a British MD, who has had stints not only as a doc in the UK, but also as a health tech and health insurance exec in the US. But now he’s at war with the system, in particular working for patients to overturn denials from insurers using AI. But what exactly is the big picture aim, and how does Warris think that he’s going to fix American health care? We had quite the discussion and we sort of agree, but also don’t. Great discussion and transcript is below the video–Matthew Holt
This was such a great discussion I wanted to publish the transcript. The way I do that is to copy the Youtube generated transcript and drop it into Claude to smooth it over. I then read it and if I think it’s made an error, dip back into the video and listen to what actually happened and make a correction. This is all code therefore for me saying I think this transcript is pretty accurate but it might have a bunch of AI and human generated mistakes.
THCB Spotlight: Warris Bokhari, CEO of Claimable
Continue reading…The Missing Vital Sign: Why Modern Medicine Still Won’t Measure Sleep

By COLIN LAWLOR
A patient comes in for an ordinary primary care appointment. The nurse runs through the usual checklist: temperature, blood pressure, pulse, weight, sometimes pulse oximetry. Sleep probably won’t come up. If it does, it will be a side note, and if the patient says, “not great,” what often follows is a brief look of sympathy and the familiar advice to relax a bit before bed.
That is, more or less, what sleep looks like in the most common diagnostic interaction in American medicine. Don’t worry, it is not much, if any better in any other country. The other vitals get numbers, while sleep gets small talk. Calling this a minor gap misses the point.
What the Evidence Says
Sleep sits among the strongest behavioral and physiological predictors we have for chronic illness, cognitive decline, mental health outcomes, and burnout.
Work out of Stanford recently showed that just one night of sleep data (admittedly from a hospital sleep lab), processed by a foundation model called SleepFM, could flag elevated risk across 130 disease categories with high accuracy. The outcomes on that list are not trivial and include all-cause mortality, dementia, myocardial infarction, and heart failure.
A 2025 umbrella review that pooled 29 systematic reviews found two-way, physiologically mediated links between sleep and depression, anxiety, plus a long catalog of cardiometabolic conditions.
And researchers at Washington State University published what is, so far, the longest objective description of sleep in chronic insomnia. Eight weeks of continuous, in-home measurement pointed to something clinicians have struggled to capture for years: night-to-night swings in sleep efficiency, sleep latency, and intermittent wakefulness are central to the condition. Sleep diaries and one-night lab studies kept missing that pattern.
The clinical rationale for measuring sleep is settled, but what remains unclear is whether medicine intends to behave as if it believes its own evidence.
Continue reading…Ellipsis Health
Ellipsis Health has come a long way from its roots in detecting depression via vocal biomarkers. Sage, its charming voice AI agent, is now helping health plans and care management companies directly interact with patients and members, helping them with medication reminders, program recruitment, postop follow up and much more. I spoke with two of the brains behind Sage, COO Melissa McCool and CMO Mike Aratow. We got into what she does, what she’s good at and whether the world (or at least the health care world) needs specific voice AI specialists–Matthew Holt
Schrodinger’s Co-pay
By MATTHEW HOLT
More tales of the woes of dealing with health insurance. I live in Marin County, California and one of the things that comes with that is a diagnosis of ADHD for my children. (OK, I have made that joke before but it is true!). My kids now visit a psychiatrist for more sophisticated med management than they receive at their pediatrician. We were (until recently) on a Blue Shield HMO via the Covered California exchange.
While I was at the doctor’s office, I talked to the staff. They told me I owed a $50 copay. I didn’t pay them (yet) and I went online and saw the claim
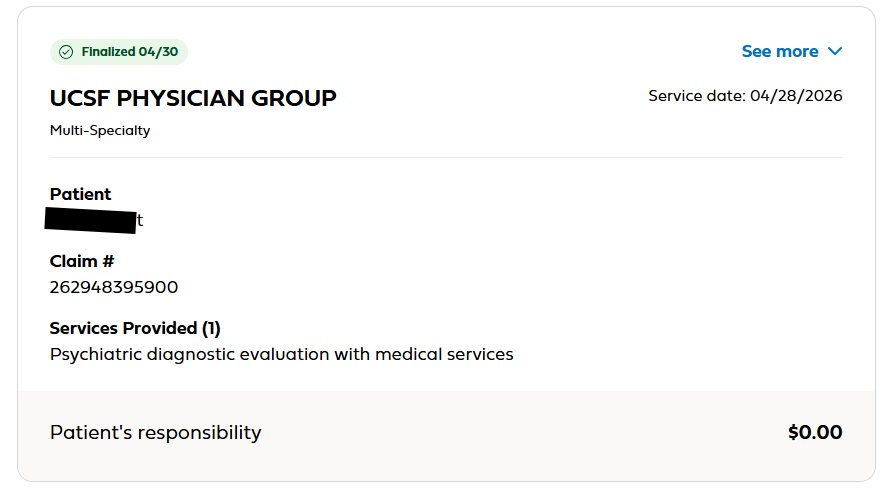
The reasonable, informed consumer might think that I owed nothing. The clue being that
“Patient Responsibility” was $0.
But if you click the “See More” in the top right it shows you this
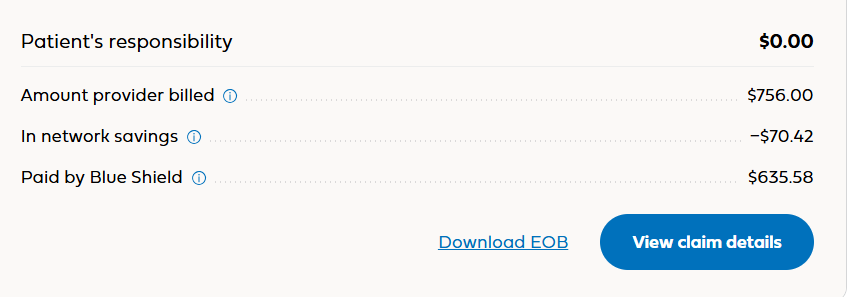
You probably still think that I owe $0. But if you add the numbers on the right you might notice they don’t total $0.
Continue reading…Dor Skuler, Intuition Robotics: Meet ElliQ
Dor Skuler is CEO of Intuition Robotics the maker of ElliQ — a remarkable AI robot that is a companion for seniors. I had a lot of fun meeting ElliQ and asking Dor about how she works. This is a wide-ranging interview with Dor and with ElliQ. She tells us about Florence Nightingale, what Dor should do with his kids and really gives you the idea of how she relates to seniors. There’s a ton of capabilities–you really have to watch the whole thing–but the end result is that Medicaid plans including NY and Washington State have determined that ElliQ allows people to stay at home longer and saves $$ on nursing home care. A fascinating view into the present and the future of how AI and robotics is changing the world–Matthew Holt
Healthcare ‘quality’ is broken. Here’s how to fix it.

By OWEN TRIPP
For decades, quality in healthcare has been defined on industry terms — not people’s terms. New technology and innovative health plan designs are finally changing that.
People know quality when they see it, and they are definitely not seeing it in healthcare. Fifty-six percent of Americans rate the quality of care as “poor” or “fair,” and 90% believe we’re overpaying for it. Likewise, 80% of employers — collectively the largest purchasers of healthcare in the country — say that higher-quality care is a top priority for their workforce.
And yet, the U.S. healthcare system remains a global leader; a lack of know-how or quality control isn’t the problem. The problem is the wide gap between how the healthcare industry has historically defined quality and how quality is experienced by the people actually receiving and paying for care.
For the past 75 years, healthcare quality has been shaped by a grab bag of federal agencies, accrediting bodies, medical organizations, health insurers, and — more recently — consumer-focused ratings outfits ranging from U.S. News & World Report to Zocdoc. Though many pay lip service to patient experience, none has clearly defined quality — or explained it intuitively enough — to help individuals make smarter healthcare decisions based on their clinical and financial context.
Healthcare needs to move beyond narrow metrics and top doc lists to create a dynamic, value-driven view of quality that consistently connects people to the best care for them, where and when they need it — and ideally, even before they know they need it. Too often, “quality” equates to some numbers on a dashboard, when it needs to be more like a combination of GPS and driver-assist technology: guiding people to their health goals, keeping them in the highest-quality lane, and nudging them if they start to drift.
This was always the vision (for some of us). But we simply haven’t had the right mix of technology and system-wide connectivity to bring it to life. Now we do.
Continue reading…






