
By ANISH KOKA
I was listening to a conversation between two critical thinkers I respect greatly: geneticist/technologist/blogger Razib Khan and Washington Post columnist Megan McArdle. Their discussion was a freewheeling rant about the problems they see with the rise of populism on the left and right, but a throwaway comment related to the US physician shortage in the context of needing high skilled immigrant labor towards the end of the almost two-hour conversation made me realize how little people really know about healthcare in America. Of course, everyone knows certain aspects of healthcare as a consumer very well, but even if you are a high-IQ individual who can make use of the vast information at all of our fingertips, it is hard to really know what the reality on the ground is without living it / having deep knowledge. Interestingly enough, early on Megan and Razib both acknowledge the impossibility of commenting on the situation in Iran, because the Iraq war taught them the folly of making conclusions from the available information. Bottom line, it doesn’t matter how smart you are if your conclusions are based on reading Colin Powell on the weapons of mass destruction Saddam Hussein must have. The public may not realize it, but health policy has a similar problem. The vast majority of academics “covering” American health policy, and in charge of describing healthcare, are ideologues whose main goal is not to describe reality, but to fashion a story. And as any screenwriter will tell you — do not let the facts get in the way of a good story.
What follows is an examination of what happens when you pull one of the important healthcare threads that forms the bedrock of many healthcare opinions that smart people like Megan and Razib hold: Rural access to healthcare in America.
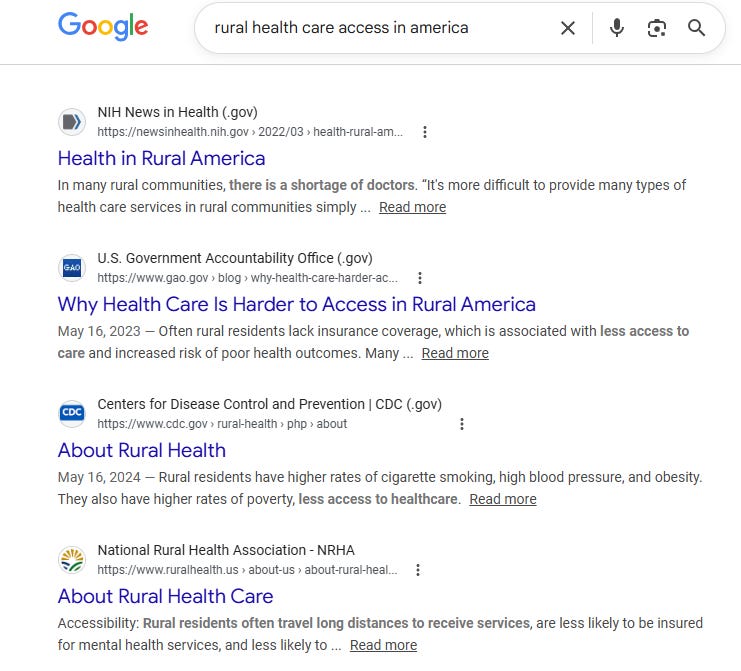
First, here’s what a Google search reveals — and notice the sources. I assure you that PubMed is not much different. Rural healthcare access in America must be bad, right?
Once we establish that healthcare access in rural America is “bad”, there are all sorts of conclusions that are downstream from that like funding of rural hospitals, and management of the physician labor supply.
But the strange thing about the rural healthcare access problem that should strike anyone over a certain age that has followed/lived healthcare is that we have been talking about this and passing legislation on the matter forever, and yet if you are to believe those who should have the most knowledge about these things, we continue to fall short.
Continue reading…











