I’m back. After the takeover editions, I’m answering Jessica DaMassa about Atul Gawande as the CEO of the ABC new venture, the demise of Caresync, Ooda Health and its demand for a female VC, and whole bunch more blather! — Matthew Holt
Adjusting for Risk Adjustment

Risk adjustment in health insurance is at first glance, and second, among the driest and most arcane of subjects. And yet, like the fine print on a variable-rate mortgage, it can matter enormously. It may make the difference between a healthy market and a sick one.
The market for individual health insurance has had major challenges both before and after the Affordable Care Act’s (ACA’s) risk adjustment program came along. Given recent changes from Washington, like the removal of the individual mandate, the market now needs all the help it can get. Unfortunately, risk adjustment under the ACA has been an example of a well-meaning regulation that has had destructive impacts directly contrary to its intent. It has caused insurer collapses and market exits that reduced competition. It has also led to upstarts, small plans and unprofitable ones paying billions of dollars to larger, more established and profitable insurers.
Many of these transfers since the ACA rules took effect in 2014 have gone from locally-based non-profit health plans to multi-state for-profit organizations. The payments have hampered competition not just in the individual market, which has never worked very well in the U.S., but in the small group market, which arguably didn’t need “help” from risk adjustment in many states.
The sense of urgency to fix these problems may be dissipating now that the initial rush for market share under the ACA is over and plans have enough actuarial data to predict costs better. There has been an overall shift to profitability. But it would be a serious mistake to think that just because fewer plans are under water, the current approach to risk adjustment isn’t distorting markets and harming competition.
Defining Engagement in an Age of Patient Monitoring and Data Collection

 SPONSORED POST
SPONSORED POST
If you have an innovative solution that addresses Patient Engagement and Remote Monitoring, Bayer’s Dealmaker Challenge wants to hear from you! Apply here for a shot at collaborating with the Bayer G4A Digital Health Team and participating in Dealmaker Day, an exclusive matchmaking event, October 9th in Berlin.
What is healthcare without patients? For decades physicians have been a one-stop shop for diagnosis and treatment, a trusted source. And yet it’s only been in recent years that the entire healthcare industry has woken up to the notion that patients can and should have an active role in their healthcare and the decision making process. Patients may not have a medical education or clinical experience, but they do have a strong asset going for them: intimate knowledge of their bodies and access to information only they can provide. The rise of wearable technologies over the past decade has only increased patients ability to quantify their experiences, health and otherwise. Diet, exercise, daily habits, stress levels, family life, physical environment all contribute to an overall picture of health. Yet too often, clinicians only see a slice of their patients health picture – the picture that is presented during office visits. The increased importance of tracking lifestyle data has clinicians and technologists asking themselves, How do we unlock more information in order to make better decisions and deliver better care?
The field is called Patient Engagement. And while the industry has mutually agreed upon it’s critical importance, the question remains as to what it looks like.Continue reading…
Health in 2 Point 00, Episode 33, (another!) Takeover Edition
Jessica DaMassa hosts this edition of Health in 2 Point 00 on the Italian leg of her Grand Tour of Europe. This time it’s another takeover with Roberto Ascione, CEO of Healthware dishing on innovation on the Almafi Coast, the impact of GDPR on digital health in Europe and the Frontiers Health Conference in Berlin this November. And yeah, that’s not my office in the background — Matthew Holt
Can Medicaid Expansion Survive?
Amid fresh political rancor and legal machinations in the ongoing war over the Affordable Care Act (ACA), there’s a bright spot: Medicaid. At least for now.
This matters. True to predictions made by Obama and supporters when the ACA became law (2010), it has taken years and a lot of blood, sweat and tears to get to this moment.
As a reminder, the U.S. Supreme Court in 2012 ruled that states could opt out of the ACA’s Medicaid expansion—leaving each state’s decision to participate in the hands of governors and state lawmakers.
On June 7, after a 4-year pitched political battle, Virginia became the 33rd state (plus DC) to expand Medicaid under the ACA. The Virginia expansion is projected to encompass 400,000 low-income Virginians.
The state swung in favor of expansion after Democrats gained the governorship and more seats in the legislature in 2016. But, importantly, key moderate Republicans relented.
Four other non-expansion states could join Virginia over the next year or two. They are Maine, Idaho, Utah, and Nebraska.Continue reading…
Misdiagnosis: Obamacare Tried to Fix the Wrong Things and Prescribed the Wrong Treatments



Today THCB is happy to publish a piece reflecting the learnings from Charles Silver and David Hyman’s forthcoming book Overcharged: Why Americans Pay Too Much For Health Care, shortly to be published by the libertarian leaning Cato Institute. In subsequent weeks we’ll feature commentary from the right radical libertarian zone on the political game board (Michael Cannon) and from the left (Andy Slavitt) about the book and its proposals. For now please give your views in the comments–Matthew Holt
There are many reasons why the United States is “the most expensive place in the world to get sick.” In Part 1 of Overcharged: Why Americans Pay Too Much For Health Care, we show that the main reason is that we pay for medical treatments the wrong way. Instead of having consumers purchase these treatments directly, we route trillions of dollars through third-parties payers – both government and private insurers.
Relying on third party payers has many consequences — few of them good. To start with, this arrangement removes the budgetary constraint that would otherwise cap the amount consumers are willing to spend. By minimizing the direct cost of treatments at the point of sale, third party payment arrangements alter everyone’s incentives fundamentally. Consumers no longer need worry about balancing marginal costs against marginal benefits; instead, they have an incentive to use all treatments that have any potential to help, regardless of their prices. When millions of consumers act on these incentives, total spending skyrockets and consumers collectively wind up worse off, because their fixed costs spiral upward too. Heavy reliance on third party payers creates a classic failure of collective action.
It isn’t just consumers. Providers love third party payment as well. And why not? Once providers have access to the enormous bank accounts of third party payers, the sky is the limit, at least until third party payers start setting limits on the amounts they will pay and saying no to unproven and/or cost-ineffective treatments that doctors want to provide and patients want to receive.
Not surprisingly, it has turned out to be extraordinarily difficult and politically unpopular for third party payers to set such limits. Obamacare’s appeal derives largely from two requirements: health insurance plans must accept all comers, including applicants with preexisting conditions that require expensive medical treatments; and health plans must provide unlimited benefits (i.e., no annual or lifetime spending caps). From an individual consumer’s perspective, what could be better than having access to unlimited amounts of money to spend on medical needs? From society’s point of view, though, this combination is a recipe for disaster.Continue reading…
The EBM Wars: When Evidence has a Price – The ECMO Trials (Part 2)

By ANISH KOKA
The year was 1965, the place was Boston Children’s and a surgery resident named Robert Bartlett took his turn at the bedside of a just born baby unable to breathe. This particular baby couldn’t breathe because of a hole in the diaphragm that had allowed the intestines to travel up into the thoracic cage, and prevent normal development of the lungs. In 1965, Robert Bartlett was engaged in the cutting edge treatment of the time – squeeze a bag that forced oxygenated air into tiny lungs and hope there was enough functioning lung tissue to participate in gas exchange to allow the body to get the oxygen it needed. Bartlett persisted in ‘bagging’ the child for 2 days. As was frequently the case, the treatments proved futile and the baby died.
The strange part of the syndrome that had come to be known as congenital diaphragmatic hernia was that repairing the defect and putting the intestines back where they belonged was not necessarily curative. The clues to what was happening lay in autopsy studies that demonstrated arrested maturation of lung tissue in both compressed and uncompressed lung. Some systemic process beyond simple compression of one lung must be operative. It turns out that these little babies were blue because their bodies were shunting blood away from the immature lungs through vascular connections that normally close off after birth. Add abnormally high pressures in the lungs and you have a perfect physiologic storm that was not compatible with life.
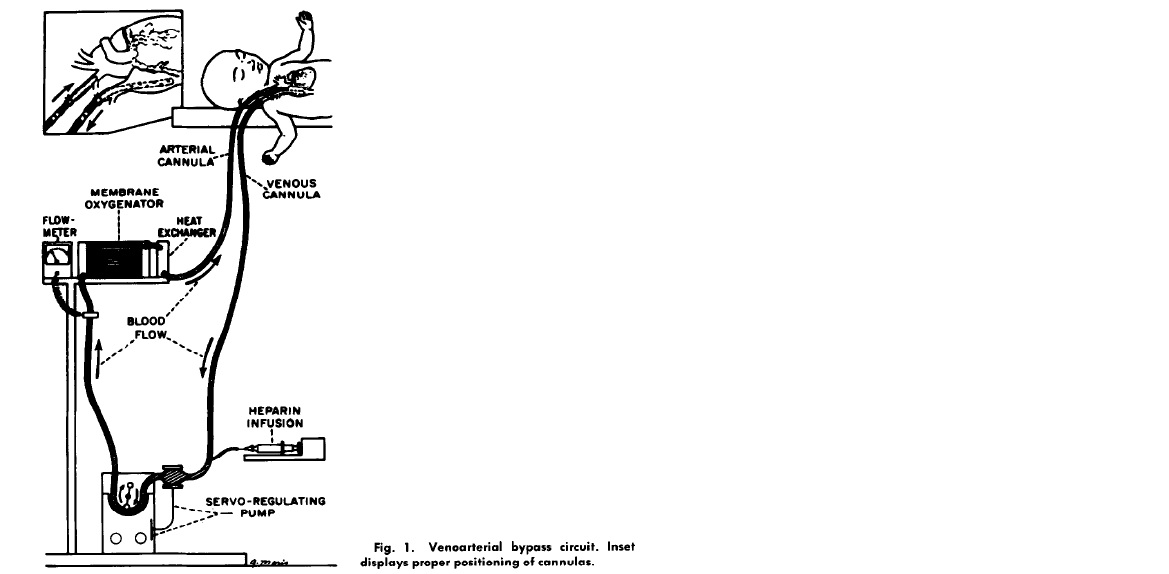
Pondering the problem, Bartlett wondered if there was a way to artificially do what the lungs were supposed to do – oxygenate. Twelve years later in 1977, while most pediatric intensive care units were still figuring out how to ventilate babies, a team lead by Bartlett was using jerry rigged chest tube catheters to bypass the lungs of babies failing the standard treatments of the day. In a series of reports that followed, Bartlett described the technique his team used in babies that heretofore had a mortality rate of 90%. A home made catheter was placed in the internal jugular vein and pumped across an artificial membrane that oxygenated blood before it was returned via a catheter to the carotid artery. The usual hiccups ensued. The animal models didn’t adequately model the challenges of placing babies on what has come to be known as ECMO (Extra Corporeal Membrane Oxygenation).
Patient 1 developed a severely low platelet count, hemorrhaged into the brain and died. Patient 2 survived but was on a ventilator for 7 weeks. Patient 3 developed progressive pulmonary hypertension and died. Patient 4 died because of misplacement of one of the ECMO catheters.
The team improved, and mortality in this moribund population improved to 20%. The pediatric journals of the day refused to publish the data because they felt ECMO for neonates was irresponsible. Once published, the neonatology community came out in force against ECMO, and some penned editorials implying the children only became supremely ill because Bartlett’s team was incompetent. The team persisted, as is anyone that is driven by the desperate need of patients. None of this should be surprising. The constant battle between skeptics and proponents is a recurring theme known to anyone with even a limited understanding of medical history. But this is where the story goes off the rails.Continue reading…
The EBM Wars: Manufacturing Equipoise (Part 1)
By ANISH KOKA
The phone rings. It’s not supposed to be ringing. It’s 2 am. The voice on the other line is from an apologetic surgery resident.
Resident: There is this patient..
Me: Yes, go ahead. Please.
Resident: He’s tachycardic.
Me: How fast?
Resident: 160 ?
Me: What’s the blood pressure?
Resident: 130/90
Me: Rhythm?
Resident: An SVT I think.. I gave adenosine. Nothing happened
Me: Audibly groaning. I’ll be in..
Forty five minutes later I’m at the bedside of a decidedly ill appearing man.
I want to be triumphant that his heart rate is only 145, and a quick glance at the telemetry monitor above his bed uncovers juicy p waves in a cadence that suggests this is no primary electrical arrhythmia.
Something is very wrong somewhere – the heart in this case is an innocent bystander being whipped into a frenzy to compensate for something.
At the moment the whip is a norepinephrine infusion being used to keep his blood pressure up.
I ask the nurse if the amount of norepinephrine infusing has been stable. She replies that his dose has been slowly escalating.
Eureka! I think – the heart rate response in this case is being driven by the norepinephrine – a powerful adrenaline that acts on beta receptors and alpha receptors within the body that increase heart rate and constrict the blood vessels to raise blood pressure. Fix the cause of the low blood pressure, come down on the norepinephrine, and perhaps the heart rate would be better.
But it turns out this particular post surgical patient doesn’t have a medical cause of low blood pressure I can find. I cycle through cardiac ultrasounds, blood gases, steroid and volume challenges, and try inching down on the norepinephrine.
All of it is to no avail. I’m growing more and more convinced this problem is surgical in nature. Perhaps an infarcted piece of bowel? All I know is that the man acts like he has no peripheral vascular tone.
An interesting thing happens shortly after. The norepinephrine drip runs out.
As one nurse runs to get another bag from the pharmacy – a quick cascade of events unfolds.
The brisk upstroke from the arterial line that marks the pressure wave generated with every beat of the heart starts to dampen. The color seems to visibly drain from the patients face, and he begins to complain that his vision is getting blurry. His systolic blood pressure is 70 – an almost forty point drop within a minute of the norepinephrine running out.
Health in 2 Point 00 Episode 32 — Takeover Edition
It’s a #Healthin2Point00 #Takeover edition — in which I get the boot and Jessica DaMassa invites Eugene Borukhovich who runs Bayer’s Digital Health Division and oversees the #Grants4Apps program to answer all he knows about ICEE Health (the conference they’re at), startups in Romania & biotech in China in just 2 minutes — Matthew Holt
Health for coins, not dollars ;) – The “not so serious” Mapping of Healthcare Cryptocurrencies

At this years’ SXSW it was all about blockchain and cryptocurrencies, but it was like that at HIMSS, JPM, CES, etc. as well. Since we wrote already about the first of the two buzzwords – blockchain as a trend in Healthcare, we decided to tackle the idea of cryptocurrencies in healthcare. First, we checked around the office and found out that several devs have been in a couple of Telegram chat rooms as they tried to buy “health coins” in a presale (ICO – initial Coin Offering; Pre-ICO).
Will you be buying your next health plan with ethereum? Or is the new health coin going to solve the problem of fragmented healthcare records?









