“So far AI in health care is being used to drive existing profits on workflows and increase revenue per event that patients in the end have to pay for. That’s not a win for anyone long term!” Included Health’s CEO Owen Tripp dives into the present and future use of AI, LLMs, patient self-triage and self treatment and all that. Another interesting conversation on where patient facing AI will end up — Matthew Holt
You’ll recall we left it with a mystery $34.94 bill which didn’t either fit the official $50 copay amount I have, nor the $0 patient responsibility in my EOB. I got a call from Rhea Fleming, an experienced customer rep at Labcorp, on whose virtual desk this has been dumped. We had a lovely conversation in which we agreed that the co-pay should either have been $50 or $0 but that it’s possible that the co-pay is the lower of $50 or the amount Labcorp was trying to collect.
She had previously called the Blue Shield of California provider line to try to figure this out. Blue Shield had indeed kicked this claim from Labcorp to Brown and Toland the IPA I am assigned to in the HMO product I bought. The charges from Labcorp were $322.28 and the response from B&T was that the contractual price (i.e. what they agreed to pay Labcorp for those tests) was $34.94, hence the “adjustment” of $287.34. However in Labcorp’s system the algorithm interpreted B&T’s response as saying 1) the agreed payment is the $34.94 according to the contract and 2) they were not going to pay so the patient owes the difference. When Rhea Fleming asked Blue Shield’s rep why the patient owed payment on this, the Blue Shield rep said that the procedure code and diagnosis code from my PCP (One Medical) did not count as preventative care. In other words Labcorp has not got paid at all for running these tests so far, because they are according to B&T “not preventative”. Although IMHO, CMS says that they are. And of course as it says my copay is $0 I’m interpreting Blue Shield of California’s EOB as saying that to me!
Hence Labcorp generated the bill for the $34.94 and sent it to me. Which started this whole telenovela.
BTW Rhea’s conclusion was that as none of the tests were “preventative,” Labcorp billed me the $34.94 as that was the total it was contractually owed rather than the $50 copay I am supposed to pay for lab work. I actually checked back in my Labcorp account and found that last year I did in fact pay $50 so perhaps last year I had different tests or somehow they have changed the algorithm. I checked the EOB for that 2024 bill and the total charge was $445.20 of which Blue Shield paid $28.07. No I couldn’t find the Labcorp bill on their system, presumably because I have paid it! Given that I paid $50 for services from Labcorp on that date (yes, it took me 7 months to pay up!), it’s likely that the agreed payment was $78.07 ($50+$28.07) of which I unthinkingly paid the $50 copay. And yes that should have been preventative too. (Perhaps I should ask for that $50 back!!)
BRIEF UPDATE: Rhea from Labcorp looked into this 2024 bill and that is exactly what happened
Then, I had another thought.
It turns out that the lab results this year generated a further concern in my doctor’s mind. (Bear in mind I had the lab tests before the office visit so that we could discuss the results). It seems that my iron levels were a little low, so while I was in the doctor’s office he ordered some more tests specifically about that. As One Medical has techs on site they drew my blood then and there and shipped it to Labcorp.
According to my EOB, Labcorp’s charge for those new tests was $60.79 of which Blue Shield or rather Brown and Toland again paid $0 and created an EOB which again said my patient responsibility was $0. I asked Rhea to check that bill in her system and it turns out that I do NOT owe Labcorp anything on that set of tests. Maybe they were coded as preventative? I tried to find the bill on my patient portal at Labcorp but because I don’t owe anything I haven’t been sent an invoice and without an invoice number you cannot check the bill!
When Rhea ended the call with me, her next move was going to enquire of Blue Shield and Brown and Toland what the reason was for me owing $0 on that bill!
Meanwhile I await the result of the official Blue Shield investigation with interest. Of course this might just have come down to Amazon One Medical coding the tests incorrectly. But it’s all fun and games if you have unlimited patience in American health care.
This is Part 2 of Jason and Gigasheets’ investigation into the Capital Women’s Care vs UnitedHealthcare contract dispute in which (partially at my request) he expanded the investigation to look at other providers in the same market. Revealing stuff!–Matthew Holt
While Capital Women’s Care (CWC) battles UnitedHealthcare over contract terms, a deeper look at Maryland’s OBGYN market reveals a complex competitive landscape where negotiated rates vary dramatically across providers and procedures. By analyzing price transparency data from both UnitedHealthcare and CareFirst BlueCross BlueShield, we can see exactly what each insurer pays CWC’s competitors. The results are eye-opening.
The Players in Maryland’s OBGYN Market
Our analysis focuses on four OBGYN providers in Maryland that have contracts with both UnitedHealthcare and CareFirst. These four practices were selected as a representation of the broader market because they have published rate data with both insurers, allowing for direct comparisons. However, Maryland’s OBGYN landscape includes dozens of additional providers, from solo practitioners to hospital-based practices, each with their own negotiated rates that may follow different patterns.
The four providers in our analysis include:
Capital Women’s Care – The large practice at the center of the UHC dispute, with multiple locations across the region
St Paul Place Specialists (Mercy Medical Center) – Baltimore-based OBGYN practice with established market presence
Maryland Physicians Edge – Women’s health group with OBGYN services, now part of Advantia
Simmonds, Martin & Helmbrecht – Established OBGYN practice, also under the Advantia umbrella
The four-provider sample provides valuable insights into competitive dynamics among major market players and helps contextualize the CWC-UHC dispute within broader industry patterns.
Following our analysis in Part 1, we examined negotiated rates for three common gynecologic procedures:
Code 56515: Destruction of cervical lesion (treatment following abnormal Pap smears)
Code 57288: Sling operation for stress incontinence (surgical procedure)
Code 58558: Hysteroscopy with sampling (diagnostic procedure for abnormal bleeding)
The Rate Comparison: UHC vs CareFirst
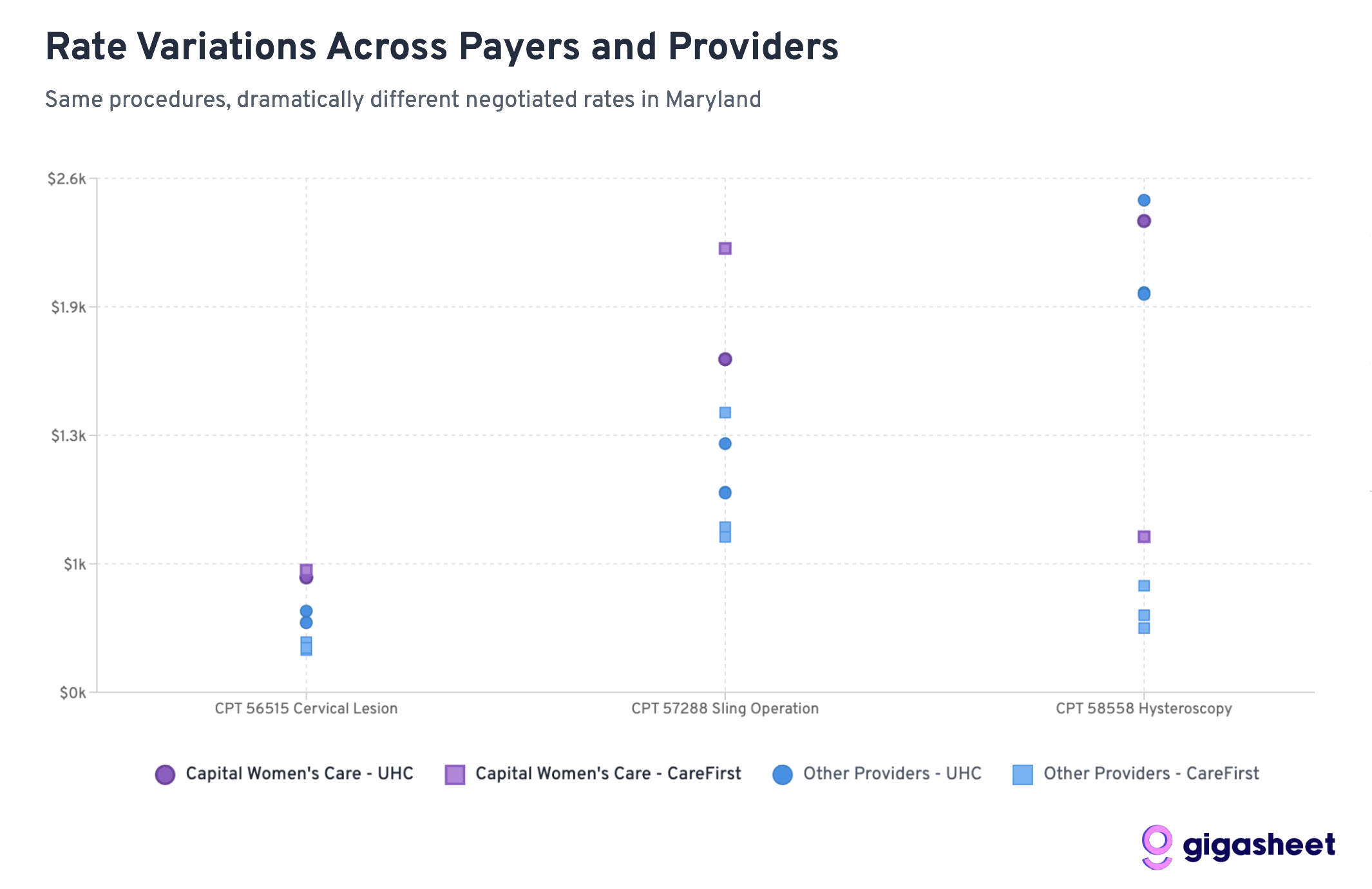
Rate variations in the price transparency data reveals a complex competitive landscape where UHC pays 200-500% more than CareFirst for hysteroscopy procedures across all providers in our sample, while Capital Women’s Care shows mixed positioning. Sometimes Capital Women’s Care commands premium rates from UHC (codes 56515, 57288), other times they’re receiving comparable rates to smaller competitors (code 58558). The data suggests both sides in the CWC-UHC dispute have legitimate arguments: CWC already receives competitive or premium compensation, while rate inconsistencies across procedures indicate room for negotiation.
Extreme rate variations (up to 519%) between UHC and CareFirst reveal market complexity, with Capital Women’s Care showing mixed competitive positioning that supports both sides’ arguments in their contract dispute.
Key Findings: A Tale of Two Insurance Strategies
UHC Generally Pays More Than CareFirst
Across 12 provider-procedure combinations, UnitedHealthcare pays higher rates than CareFirst 75% of the time. This suggests CareFirst has been more aggressive in negotiating lower rates across the Maryland market.
Hysteroscopy Shows the Most Dramatic Differences
For Code 58558 (hysteroscopy with sampling), the rate differences are staggering:
UHC pays 203-519% more than CareFirst across all providers
Average UHC rate: ~$2,200 vs CareFirst rate: ~$510
This represents the largest systematic difference across procedures
Capital Women’s Care Commands Premium Rates
CWC’s rates relative to competitors reveal why UHC may be resistant to further increases:
Code 58558: CWC’s UHC rate ($2,384) is already comparable to competitors, despite CWC’s larger scale
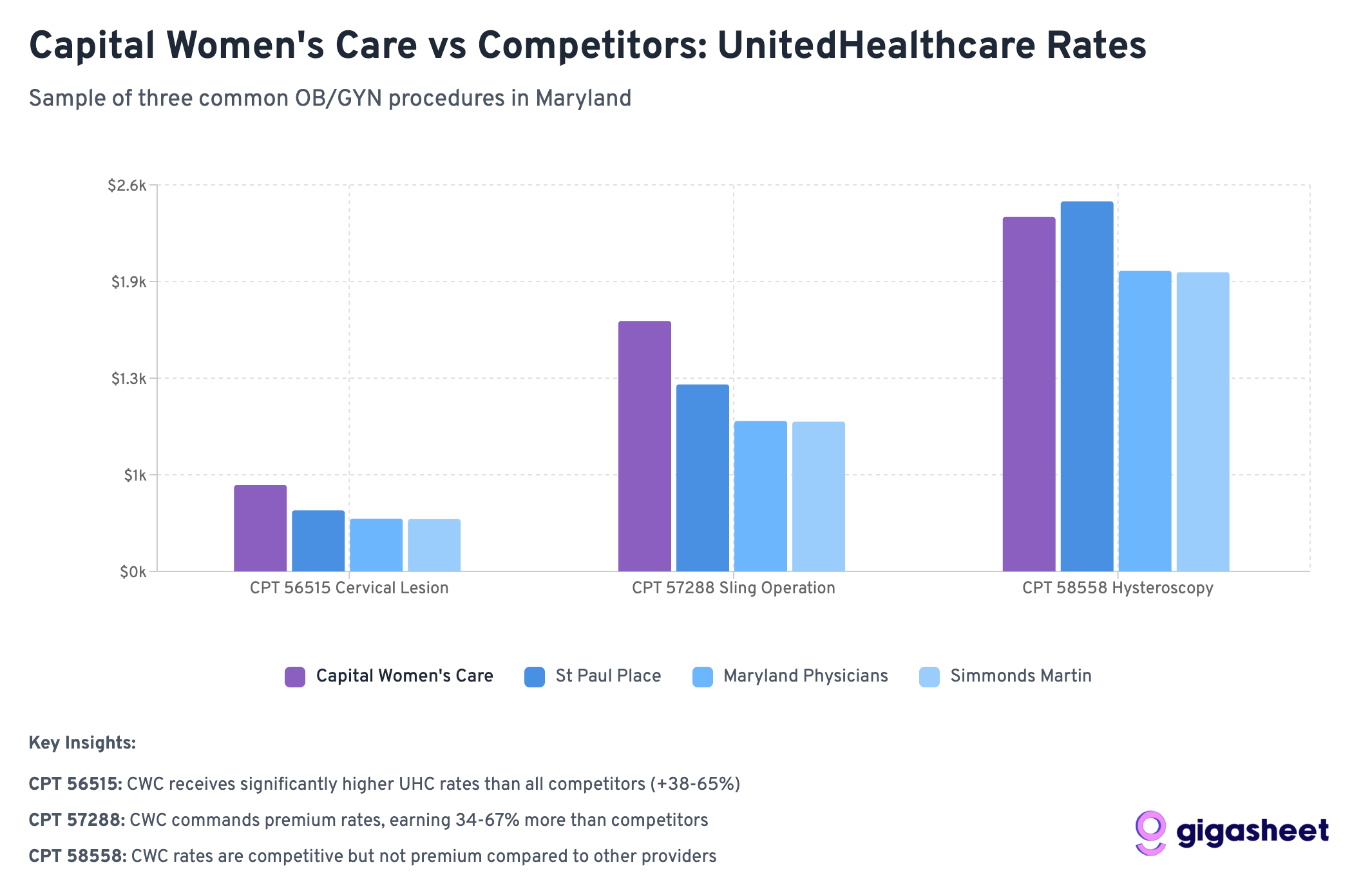
Code 56515: CWC gets slightly better terms from UHC ($581) vs competitors ($352-411)
Code 57288: CWC receives significantly higher rates from UHC ($1,685) vs most competitors ($1,008-1,258)
Wide Rate Variations
The most extreme example: Simmonds Martin & Helmbrecht receives 519% more from UHC than CareFirst for hysteroscopy procedures (a difference of nearly $1,700 per procedure). These patterns suggest that while some procedures have established market rates, others (particularly diagnostic procedures like hysteroscopy) lack standardized pricing, contributing to the complexity of provider-insurer negotiations like the CWC-UHC dispute.
Rate variations reveal dramatic pricing inconsistencies across Maryland’s OBGYN market, with hysteroscopy procedures showing the most extreme disparities difference between the highest and lowest negotiated rates for identical services.
What This Means for the CWC-UHC Dispute
CWC Already Commands Premium Rates
The data reveals a key insight: Capital Women’s Care isn’t necessarily getting unfair treatment from UHC. In fact, CWC often receives higher rates than competitors from both insurers:
For hysteroscopy (58558), CWC gets comparable UHC rates despite being a larger practice that should theoretically have less negotiating leverage
For cervical procedures (56515), CWC receives 40-65% higher rates from UHC than smaller competitors
For sling operations (57288), CWC’s UHC rate ($1,685) significantly exceeds most competitors
This pattern suggests UHC’s resistance to further rate increases may be economically rational rather than punitive.
Industry-Wide Rate Fragmentation
The massive variations between UHC and CareFirst rates across all providers highlight fundamental pricing inefficiencies in healthcare. However, within each insurer’s network, CWC consistently commands premium rates, suggesting their market position is already strong.
Scale vs. Negotiating Power
Conventional wisdom suggests larger practices should receive lower per-unit rates due to volume efficiencies. The data shows the opposite: CWC often receives higher rates than smaller competitors, indicating they’ve successfully leveraged their size for premium pricing rather than volume discounts.
The Broader Market Dynamics
CareFirst’s Market Power
CareFirst BlueCross BlueShield appears to have leveraged its position as Maryland’s dominant insurer to negotiate significantly lower rates across the board. With roughly 50% market share in Maryland, CareFirst can drive harder bargains with providers who can’t afford to lose access to half their potential patient base.
UHC’s Perspective Becomes Clearer
UnitedHealthcare’s position in the dispute gains context when viewed against competitor rates. UHC is already paying CWC premium rates compared to other Maryland OBGYN providers. From UHC’s perspective, further rate increases would create an even larger gap between what they pay CWC versus smaller practices.
The Economics of Provider Consolidation
The data illustrates a key tension in healthcare consolidation: large practices argue their size justifies higher rates due to quality and convenience, while insurers worry about paying premium prices for what should be commodity services. CWC appears to have successfully established premium pricing, making UHC’s resistance to further increases economically understandable.
Looking Forward: What This Means for Healthcare Costs
The Price Transparency Revolution
This analysis is only possible because of federal price transparency requirements that took effect in 2021. For the first time, we can see exactly what insurance companies pay different providers for the same services, revealing the massive hidden variations in our healthcare system.
Market Efficiency Questions
The data raises fundamental questions about market efficiency:
Why does the same procedure vary by 500% between insurers at the same provider?
Are patients getting better care when insurers pay more, or are some insurers simply paying inflated rates?
How can patients make informed decisions when rate variations are this extreme?
Regulatory Implications
These findings may attract regulatory attention, particularly around:
Whether rate variations this extreme serve any legitimate purpose
How to ensure patients aren’t penalized for insurance-provider rate disputes
Whether price transparency alone is sufficient to drive market efficiency
Conclusions: Both Sides Have Valid Arguments
The Capital Women’s Care vs UnitedHealthcare contract dispute becomes more nuanced when viewed through competitive rate data. Our analysis reveals that both sides can point to legitimate evidence supporting their positions:
Capital Women’s Care’s Case:
Rate Inconsistencies: For some procedures like hysteroscopy (58558), CWC receives similar UHC rates to much smaller competitors, despite CWC’s larger scale and presumably higher overhead costs.
CareFirst Comparison: CWC’s significantly higher rates from CareFirst for certain procedures (like sling operations at $2,245 vs UHC’s $1,685) suggest room exists for UHC rate increases.
Market Position Justification: As Maryland’s largest OBGYN practice, CWC can argue their scale, convenience, and comprehensive services warrant premium compensation.
UnitedHealthcare’s Case:
Already Premium Rates: Across multiple procedures, CWC receives higher rates from UHC than smaller competitors (40-65% higher for cervical procedures), indicating UHC already recognizes CWC’s value.
Economic Reasonableness: Further rate increases would create an even larger premium gap between CWC and other providers, potentially making UHC’s network economics unsustainable.
Mixed Performance: The inconsistent pattern across procedures suggests CWC’s premium positioning isn’t uniformly justified across all services.
The Complexity of Healthcare Negotiations:
Rather than a clear case of unfair treatment, the data reveals the inherent complexity of healthcare rate negotiations. Both parties can legitimately point to specific procedures and comparisons that support their position, while the overall picture remains genuinely mixed.
This analysis suggests the dispute reflects broader challenges in healthcare pricing: How do you fairly compensate scale and market position while maintaining reasonable cost structures? The competitive data shows there’s no obvious “right” answer; just different ways to interpret the same complex market dynamics.
The real insight isn’t that one side is clearly right, but that healthcare rate negotiations involve legitimate competing interests where reasonable people can look at the same data and reach different conclusions about fair compensation.
Jason Hines is CEO of Gigasheet which delivers AI-powered price transparency market intelligence.. This was first posted on their corporate blog
Note: This analysis is based on a sample of price transparency data filed by UnitedHealthcare and CareFirst BlueCross BlueShield, as mandated by federal regulations. The rate calculations are aggregations of data from multiple contracts and locations within each provider organization. To expand our rate analysis from Part 1, we resolved EINs to organization names using public data sources.
(I copied this here from Linked in where it 65+ comments just so I can find it when the story continues) Too painful to write up fully but I am on my 4th transfer in one phone call to MarinHealth trying to get an echocardiogram (EDIT-not an EKG as I originally wrote). They have lost the referral from One Medical twice. I had to download the referral and email it to them (Lucky it’s on the One Medical system). Every person has asked for my DOB and phone number. The guy who got the email, read the referral and transferred me. The latest guy appears very puzzled & wants me to fax him the referral. Eventually he gets me to his supervisor who says that radiology & cardiology are separate and they can’t receive an email because it’s a HIPAA violation. (I claimed to be Lucia Savage & laughed at him). Now I have to figure out how to fax it to them and the supervisor promised to call me back. He had to ask for my phone number….
Oh and I can’t book a echocardiogram on MyChart, but I can book a mammogram.
I’ll follow up in the comments. BTW that phone call was 19 minutes
UPDATE: OK, so I faxed them via a dodgy efax company whose “free trial” I need to remember to cancel. The supervisor did call me back, but for some reason my phone didn’t ring! He left a message and booked an appointment for me. But not in their Marin facility. In the next county over! (And Sonoma is very lovely). A 45 min drive rather than a 10 min drive from my house. I can SEE the appointment in the UCSF MyChart, and I can cancel it. but I cannot request a change or see when I could book one closer to me (presumably at a later date). So I guess I will call back on Monday….
UPDATE: So I called back today and got the appointment changed to the closer location. I had to wait one more day… I know you are all on tenterhooks so I will tell you if my heart works in 2 weeks!
UPDATE to the Update. A human called me and cancelled my appointment. Apparently the tech was out sick. Still no word on whether I have a heart or just a black pit inside my chest
UPDATE: I finally got in and had the Echocardiogram. Marin Health had an iPad based fast check in (well done). I didn’t recognize whose software it was. The echocardiogram took 45 minutes and was a bit like having somone stick their finger in your chest the whole time. Yes I do have a heart! More to come
My friend Rosemarie Day joins me to talk about the Healthcare Leaders for Democracy session coming up on September 4 (Thursday) at 8pm ET 5pm PT. It’s a one hour session with Atul Gawande as the keynote speaker, joined by Don Berwick and John McDonough. It’ll be a fascinating discussion and it’s a fundraiser for Movement Voter Project, but it’s free to sign up.
Rosemarie and I talked about how we work on getting grassroots mobilization for the mid-terms and beyond, and we hope people will come and join.
On August 1, 2025, Capital Women’s Care (CWC), one of the largest OB/GYN practices in the Mid-Atlantic region went out-of-network with UnitedHealthcare, affecting tens of thousands of women across Maryland, Virginia, Pennsylvania, and Washington D.C. The contract dispute between Capital Women’s Care (CWC) and UnitedHealthcare offers a fascinating case study in how price transparency data can illuminate the real dynamics behind these high-stakes negotiations.
The Public Battle
Capital Women’s Care, with more than 250 physicians and healthcare professionals, confirmed that its agreement with UnitedHealthcare would lapse despite ongoing negotiations. The practice urged patients to contact UHC to voice their concerns about losing access to their providers.
UnitedHealthcare fired back with detailed public claims on their website, alleging that CWC “refused to move off its demands for double-digit price hikes” and is “significantly higher cost today compared to peer providers throughout Maryland and Virginia”. UHC provided specific examples, claiming that a vaginal delivery from CWC would cost “more than 120% higher – or over $2,600 more – than the average cost of other OB/GYN providers”.
But what does the actual price transparency data reveal about these competing claims?
What the Transparency Data Shows
Using Capital Women’s Care’s negotiated rates from UnitedHealthcare’s own machine-readable files, we analyzed a sample of common OB/GYN procedures from Maryland rate data. While this represents only a subset of all procedures and focuses specifically on Maryland rates, it provides valuable insights into the real payment dynamics between these organizations. The data paints a more nuanced picture than either party’s public statements suggest.
Data Methodology Note: Our analysis examined negotiated rates for Capital Women’s Care from publicly available machine-readable files, focusing on Maryland providers and filtering out statistical outliers (rates below 50% or above 500% of Medicare). We analyzed rates for both UnitedHealthcare and CareFirst across three common OB/GYN procedures where both payers had sufficient data.
CWC’s Rate Position vs Other Payers
Our analysis of three common OB/GYN procedures in Maryland reveals that CWC’s rates with UnitedHealthcare were actually quite competitive compared to other major payers:
Negotiated rates for three common OB/GYN procedures show UHC was paying competitive rates compared to CareFirst
For the three procedures where both UHC and CareFirst have negotiated rates with CWC:
This sample data suggests UnitedHealthcare was already getting favorable rates from CWC compared to other major payers, calling into question UHC’s claims about CWC being “significantly higher cost.”
The Medicare Benchmark Reality
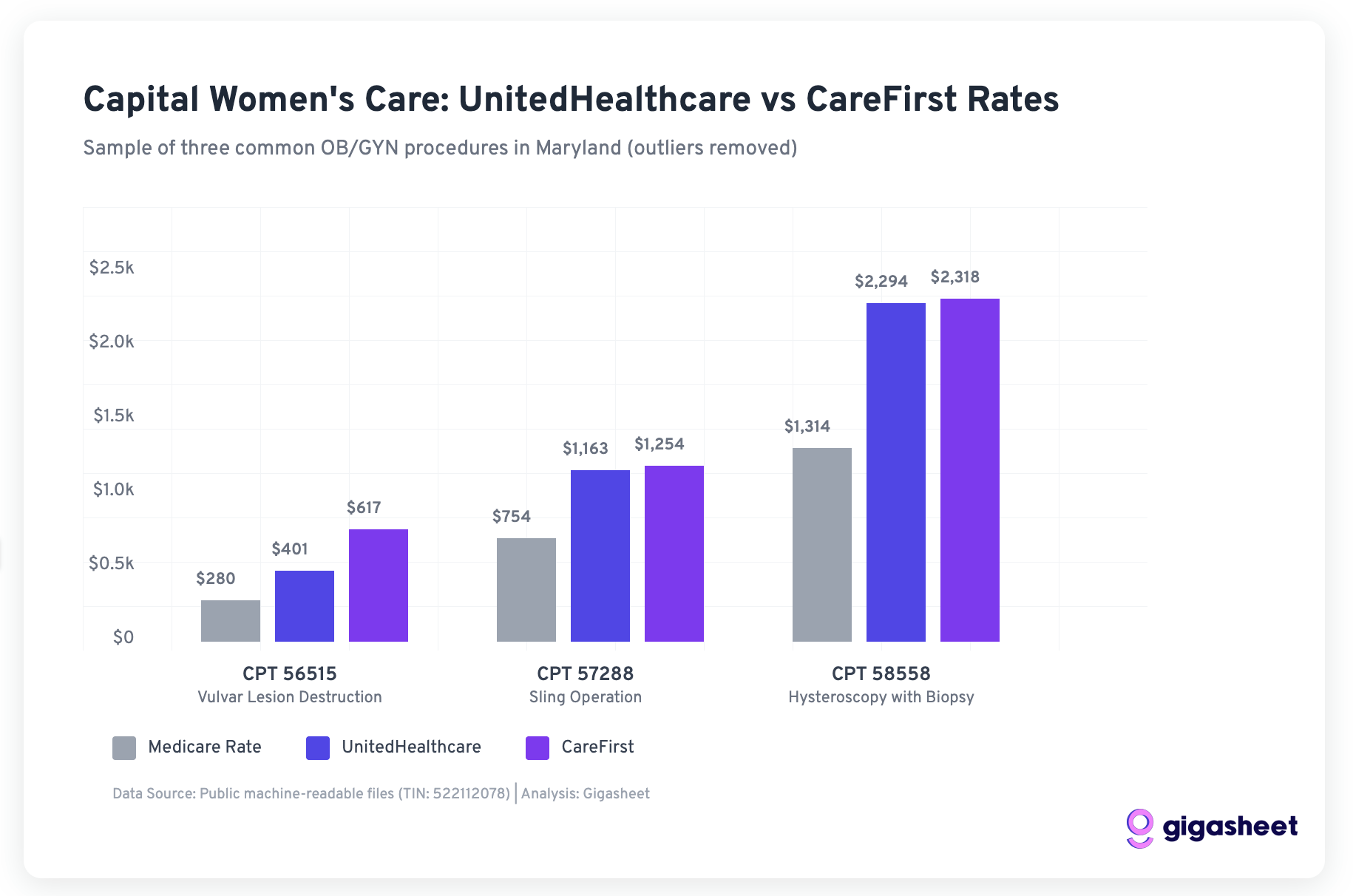
Both UHC and CareFirst were paying CWC rates well above Medicare in our sample:
UnitedHealthcare: 143-175% of Medicare rates
CareFirst: 166-220% of Medicare rates
While CareFirst paid higher rates, UnitedHealthcare’s rates were still substantial premiums over government reimbursement, suggesting the “double-digit increases” CWC requested may have been attempts to align with market rates other payers were willing to pay.
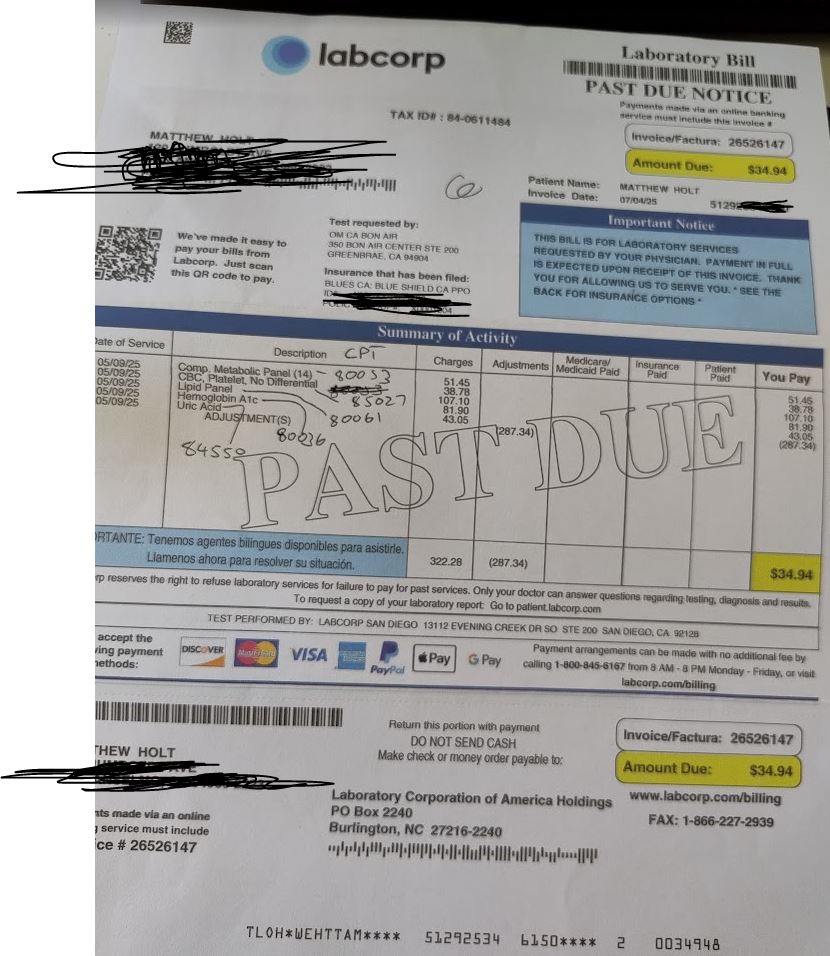
Over the weekend Labcorp sent me a final due notice on my bill…. the one that they couldn’t tell me about without asking for all the information they already had.
I call Labcorp customer service in the Philipinnes. The friendly rep says that they have had a message saying that “the insurance company requires that Labcorp provides documentation from the ordering physician”. What documentation, I ask? A letter that tells them what the updated codes are. Given that the Brown & Toland Physicians rep told me those codes and they must have been sent them by Labcorp when Labcorp sent in the claim, that seems to make no sense. I’m not yet prepared to ask my doctor’s office to get involved in this! (Better look out though, Andrew Diamond!). So I’ll let that go for a moment.
However, Labcorp says that they received an EOB from Blue Shield of California PPO–it had my correct member number even though I am an HMO not PPO member. No the EOB did not come from the IPA Brown & Toland Physicians, and yes I asked very precisely. The EOB says the co-pay is $34.94. Labcorp can’t ascribe it to any one of the 5 individual lab tests (which all look preventative under the ACA to me but maybe one isn’t). So the $34.94 is the copay from the EOB that Blue Shield of California sent to Labcorp.
They asked me for my copy of the EOB. I sent one 5 days ago, but sent it again just to be sure.
Next up, asking Blue Shield of California what precisely they sent to Labcorp saying my co-pay is $34.94 when the one they sent me (well have on their website) says $0. Oh and by the way, the standard copay for labs on my plan is $50, not $34.94!
On my Blue Shield of California member portal there’s a message with a letter. Apparently they opened a customer grievance for me! I called the customer grievance number in the letter. According the answering IVR message there is a chat option for providers with grievances, but not one for consumers. My hold time is estimated at 20 minutes. A nice rep called Susie comes on in only 15 mins.
After verifying that she knows who I am she says there are 2 different grievances! One is an appeal for the lab test & one is a complaint about the process, both opened August 12. I suspect they were initiated by the nice man from the Executive office who called me on that day. Rep Susie is limited to telling me that appeal status. But she tells me that an appeal coordinator is looking into the complaint and will be back in touch within 30 days. AND she gives me an email to reach said coordinator at! So I sent that person an email….lets see what happens!
In previous posts in this series, we have covered the definitions of Unified Digital Health platforms and whether “EHRs can become UDHPs.” In this follow-on post, we’ll talk through the requirements for success for a UDHP and which types of healthcare organizations are best suited for which types of UDHPs. This post will build on findings from the previous posts.
The Market Needs UDHPs: Key Takeaways from Previous Posts
Key Takeaway 1: The healthcare industry needs UDHPs to create a centralized, common architecture for healthcare organizations
Key Takeaway 2: The healthcare organizations leveraging UDHPs will achieve a myriad of benefits, from competitive advantages to clinical, financial, and operational gains
Key Takeaway 3: UDHPs are not all-or-nothing or mutually exclusive from EHRs. As we explored in our last post, EHRs could expand into UDHPs. These EHRs as UDHPs (or the relative platform of platforms) may be the optimal choice for some market segments. EHRs may also be accommodated into cloud-first UHDPs.
Key Takeaway 4 / Guiding Criterion: This post will focus on US regional and local health systems and outpatient groups of all sizes.
The Approach: Market -> Segments -> Options -> Fit
For this post, we will start from the top-down market perspective, analyzing the overall market landscape.
Once we have described the landscape, we will call out the key segments (organization types, sizes, and profiles) that we will be evaluating.
At this point, we will approximate IT budgets and IT team sizes by organization type to determine capabilities of building as opposed to depending on partners and vendors.
Then, we’ll review the constraints for implementation and ownership, outlining the drivers of UDHP fit.
Next, we’ll break down the different ways UDHPs can be developed and maintained.
Leveraging an EHR as UDHP
License from UDHP vendor
“Home grown” cloud-first solution
Finally, we’ll crosswalk the segments and the optimal option for each segment, based on their specific needs and estimated IT and budgetary resources.
The Healthcare Market & Major Health System Segments
Starting with a compelling graphic from the Kaiser Family Foundation, we see a 2023 breakdown of the total US healthcare medical expenditure, totaling ~$4.9 trillion.
While the total healthcare spend that occurred in hospitals is an astounding ~$ 1.5 trillion, accounting for 31% of total healthcare spend, this leaves much of care outside the four walls of hospitals. This amount of care occurring outside of hospitals aligns with efforts to push patients into less acute care settings, emphasizing preventative, proactive medicine instead of acute, reactive medicine. As the need for UDHPs applies to more than inpatient hospitals, we will also review the other segments highlighted in the pie chart, including: outpatient clinics and practice groups, and “other health” containing services delivered at other contexts like PACs and SNFs, and Ambulatory surgical centers.
After 6 minutes I got a very confused person. BTW there is NO way to communicate with Labcorp on the website, and if you put your invoice number into their IVR system there is NO way to get a human. The only way to do that is to hang up and start again, NOT put in your invoice number and hit 0. Then wait on hold with muzak to get a human. They then ask your DOB and phone number. The call center is in the Philippines BTW.
I explained that I wanted information on which test was not covered under the ACA. Brown and Toland/Blue Shield’s EOB says I have a $0 co-pay (see image).
The Labcorp rep told me that of the 5 tests done (with CPT code and price), 3 were not covered. The Lipid (85027 $107.10), the A1C (80061 – $81.90) Uric Acid (84550 $43.05). 2 of those 3 clearly are covered under the ACA. The Uric Acid one may not be according to my reading of the CMS site. Labcorp submitted that bill to Blue Shield. The rep consistently told me the claim was sent to Blue Cross Blue Shield of CA, which doesn’t exist.
At that point — 15 minutes in — the call dropped. I don’t know if they just hung up but they had asked for my phone number. They didn’t call me back.
But I am a pain in the ass, and I called them back. After roughly 4 mins on hold, I got another rep. She told me ALL of the CPT codes/lab tests were subject to copay. She told me that Blue Shield (NOT Brown & Toland Physicians) has bundled all of these codes and there is a co pay for all of them. Which is what the bill says.
So the only thing I can do is to send an email with the screenshot of the EOB, which is from the IPA not Blue Shield. So I did that and may get a response in 3-5 business days.
I know you are on tenterhooks. Let’s see what happens next but the complete absence of anything resembling consumer transparency or access to the relevant information makes a mockery of everything Paul Markovich says on stage.
UPDATE. Labcorp both emailed me back AND asked me to contact them on Linkedin. See what they asked for! Yes even though they have sent me a bill and I sent them the invoice number, they want every detail possible about the claim they ALREADY have!
Full email below just for giggles
Oh and when I went to DM them on Linkedin as they requested their account was not accepting DMs!
2nd UPDATE: A very nice man from the Blue Shield of California corporate office called me up. We discussed whether the care I got was preventative or not and why I was being charged the $34.94. Of course he didn’t know. He agreed with me that it was a shit show, and actually started to complain that sometime HE had been charged for preventative stuff he thought should have been free.. He didn’t have any solution other than calling Brown and Toland to cancel the charge, but I told him I didn’t want any special treatment (at least not yet!). I told him I wanted no special favors, but I wanted the claim reprocessed and an explanation.
I have to admit, I’ve steered away from writing about AI lately. There’s just so much going on, so fast, that I can’t keep up. Don’t ask me how GPT-5 differs from GPT-4, or what Gemini does versus Genie 3. I know Microsoft really, really wants me to use Copilot, but so far I’m not biting. DeepMind versus DeepSeek? Is Anthropic the French AI, or is that Mistral? I’m just glad there are younger, smarter people paying closer attention to all this.
Still, I’m very much concerned about where the AI revolution is taking us, and whether we’re driving it or just along for the ride. In Fast Company, Sebastion Buck, co-founder of the “future design company” Enso, posits a great attitude about the AI revolution:
The scary news is: We have to redesign everything.
The exciting news is: We get to redesign everything.
He goes on to explain:
Technical revolutions create windows of time when new social norms are created, and where institutions and infrastructure is rethought. This window of time will influence daily life in myriad ways, from how people find dates, to whether kids write essays, to which jobs require applications, to how people move through cities and get health diagnoses.
Each of these are design decisions, not natural outcomes. Who gets to make these decisions? Every company, organization, and community that is considering if—and how—to adopt AI. Which almost certainly includes you. Congratulations, you’re now part of designing a revolution.
I want to pick out one area in particular where I hope we redesign everything intentionally, rather than in our normal short-sighted, laissez-faire manner: jobs and wealth.
It has become widely accepted that offshoring led to the demise of U.S. manufacturing and its solidly middle class blue collar jobs over the last 30 years. There’s some truth to that, but automation was arguably more of a factor – and that was before AI and today’s more versatile robots. More to the point, today’s AI and robots aren’t coming just to manufacturing but pretty much to every sector.
Former Transportation Secretary Pete Buttigieg warned:
The economic implications are the ones that I think could be the most disruptive, the most quickly. We’re talking about whole categories of jobs, where — not in 30 or 40 years, but in three or four — half of the entry-level jobs might not be there. It will be a bit like what I lived through as a kid in the industrial Midwest when trade in automation sucked away a lot of the auto jobs in the nineties — but ten times, maybe a hundred times more disruptive.
Mr. Buttigieg is no AI expert, but Erik Brynjolfsson, senior fellow at Stanford’s Institute for Human-Centered Artificial Intelligence and director of the Stanford Digital Economy Lab, is. When asked about those comments, he told Morning Edition: “Yeah, he’s spot on. We are seeing enormous advances in core technology and very little attention is being paid to how we can adapt our economy and be ready for those changes.”
You could look, for example, at the big layoffs in the tech sector lately. Natasha Singer, writing in The New York Times, reports on how computer science graduates have gone from expecting mid-six figure starting salaries to working at Chipotle (and wait till Chipotle automates all those jobs). The Federal Reserve Bank of New York says unemployment for computer science & computer engineering majors is better than anthropology majors, but, astonishingly, worse than pretty much all other majors.
And don’t just feel sorry for tech workers. Neil Irwin of Axios warns: “In the next job market downturn — whether it’s already starting or years away — there just might be a bloodbath for millions of workers whose jobs can be supplanted by artificial intelligence.” He quotes Federal Reserve governor Lisa Cook: “AI is poised to reshape our labor market, which in turn could affect our notion of maximum employment or our estimate of the natural rate of unemployment.”
In other words, you ain’t seen nothing yet.
While manufacturing was taking a beating in the U.S. over the last thirty years, tech boomed. Most of the world’s largest and most profitable companies are tech companies, and most of the world’s richest people got their wealth from tech. Those are, by and large, the ones investing most heavily in AI — most likely to benefit from it.
Professor Brynjolfsson worries about how we’ll handle the transition to an AI economy:
The ideal thing is that you find ways of compensating people and managing a transition. Sad to say, with trade, we didn’t do a very good job of that. A lot of people got left behind. It would be a catastrophe if we made the similar mistake with technology, [which] that also is going to create enormous amounts of wealth, but it’s not going to affect everyone evenly. And we have to make sure that people manage that transition.