If you follow along with my rantings on THCB, Twitter and Linkedin you’ll know that I am unhappy with America’s growing inequality, both in wealth and income. Now, there are a few signs that so long as we have full employment the income picture for the lowest paid is getting a little better. But wealth inequality is clearly not getting better.
You may remember this video explaining wealth inequality. Worth a watch if you haven’t seen it.
Well that was made in 2011. Back then Elon Musk was barely a billionaire, and more than a decade of massive stock market appreciation later, we know that the rich have gotten a lot richer, and their taxes went down following the Trump tax cuts in 2017.
Meanwhile, something similar has been going on in health care. The health economy has amazingly not taken much more of the overall economy since 2010. It went from 13% to 17% of GDP between 2000 and 2010 but has amazingly stayed around there–only popping up during the Covid recession and then heading down again. But the amount of money flowing into health care has stayed at a constant rate. And the American people continue to hate their experience with the health system.
They’re aren’t many selfless heroes. Payers, providers, doctors, pharma, equipment suppliers are all doing well. Wendell Potter has continued to show how health insurance companies have consolidated and gotten richer over the past decade plus. Big Pharma has managed the translation away from the mass market blockbusters of the 1990s to the high priced niche drugs of today, and now with GLP-1s is managing to keep those high prices. Despite lots of whining by the AHA, hospitals–which got massive handouts from the CARES Act during Covid–are all doing well again. But it’s always good to check in with the big non-profit systems. This isn’t the first time I’ve written about this. Early this year in a larger rant I wrote:
Over the last 30 years America’s venerable community and parochial hospitals merged into large health systems, mostly to be able to stick it to insurers and employers on price. Blake Madden put out a chart of 91 health systems with more than $1bn in revenue this week and there are about 22 with over $10bn in revenue and a bunch more above $5bn. You don’t need me to remind you that many of those systems are guilty with extreme prejudice of monopolistic price gouging, screwing over their clinicians, suing poor people, managing huge hedge funds, and paying dozens of executives like they’re playing for the soon to be ex-Oakland A’s. A few got LA Dodgers’ style money.
One of the things that the non-profits have to do is file the 990 form with the IRS. Among other things it shows how much money the organization’s executives make. Now it’s not like non-profit health system execs are the only ones coining it. In 2022 the biggest for-profit chain HCA’s CEO made $20m and 4 others there made over $5m. But at least HCA is a nakedly capitalist organization, and it pays taxes.
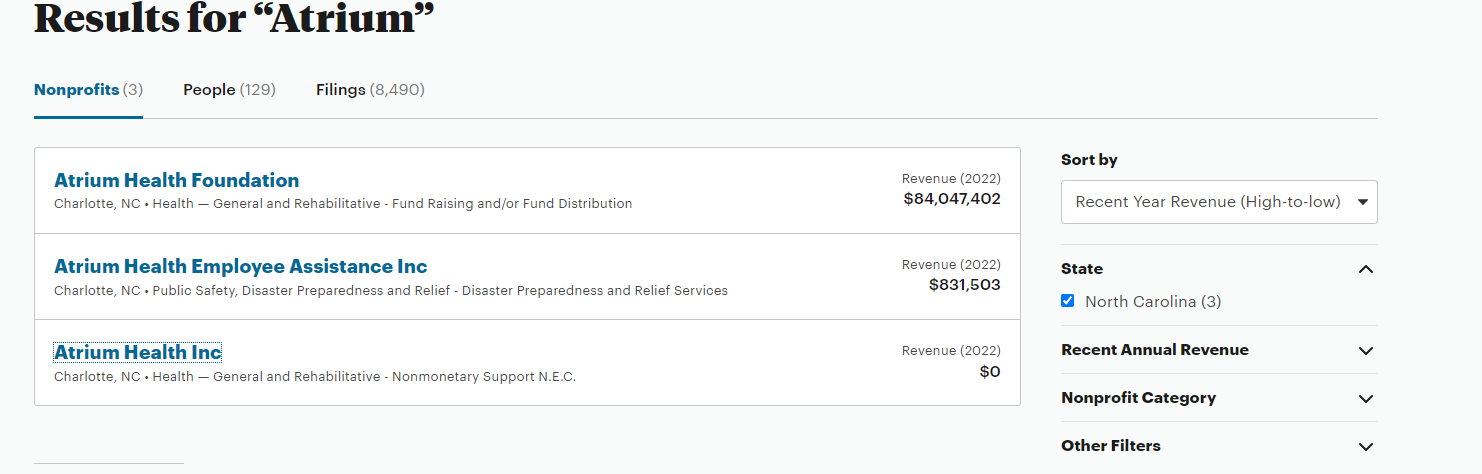
Recently one of the bigger hospital systems, UPMC put out a new 990. Unlike the previous version they put out, the 990 on their website is a photocopy that can’t be searched. Maybe that’s an accident, although any non-profit can put out an easily searchable document. For instance here’s the one from a teeny non-profit that I control. You can search the words “Reportable Compensation” and find that sadly I got paid zilch for my efforts. Not sure why UPMC can’t do the same.
Luckily for those of us who care, Propublica is a little more aggressive. They reproduced a searchable version. The way ProPublica did it was to download an xls from the IRS. One reason it’s worth looking at was that this year as opposed to 2022, UMPC didn’t post its compensation in $$ order.
I’m not knocking UPMC too much. Very few other big non-profit health systems put anything like as much effort into detailing who makes what amount on their 990s. They usually stop after the first 10-20 employees. UPMC goes down to 220+
So I copied and repasted the compensation information from ProPublica and did the necessary editing of 230 cells to be able to sort by compensation. You can find the spreadsheet here. (Feel free to copy & paste and do your own edits).
So what does it tell you?
UPMC had a CEO called Jeffrey Romoff who worked there his whole career. Romoff became President in the 1990s and took over as CEO in 2006. Using aggressive M&A, and some very sharp elbows including against the unions, Romoff essentially created the massive local monopoly that is the modern UPMC. His biggest moment in the national spotlight was when he went on 60 Minutes in 2011 and forgot his salary (he said it was $7m but then corrected it to $6m). Ten years later Romoff’s salary was a tad under $13m. If you are wondering, the median annual wage in the US in 2011 was $34,460. By 2022 it was $45,760. So the average salary increased 34% in nominal terms over that time. Romoff’s went up by more than 100%.
But that’s all well and good. Romoff retired at the age of 75 in August 2021 and was replaced by Leslie Davis.
So for the period covering July 2022 to June 2023, who was the highest paid person at UPMC?
Continue reading…



 Affordable Care Act (ObamaCare) has been knocked for its alleged unintended consequences. The bill’s attracted speculation that
Affordable Care Act (ObamaCare) has been knocked for its alleged unintended consequences. The bill’s attracted speculation that 







