By MATTHEW HOLT
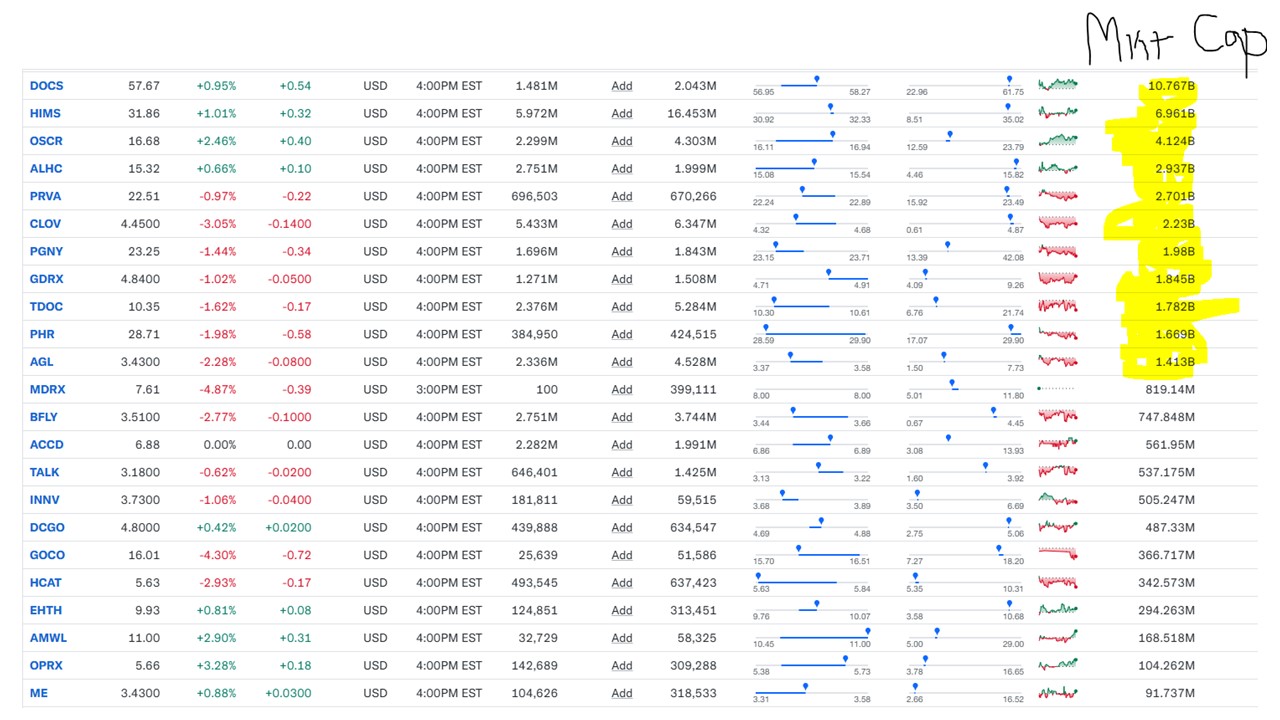
The big news in the comeback of digital health is that Hinge Health filed its S1 and is looking to go public soon. I suspect that they’d have preferred to get the IPO done late last year when the AI bubble was expanding rather than deflating, but timing the market is tough! Nonetheless Hinge is almost profitable and at over $350m in revenue at a growth clip of some 75% last year, in terms of a show pony to trot out, it’s about as good as the digital health field has got. The problem is that the last round in 2021 was at a $6bn+ ZIRP-era valuation with Tiger & Coatue paying the idiot price because Teladoc was trading at $15bn market cap then (albeit down from $30bn a year before that!). That is, err, no longer the case. There’s a bunch of weirdness in the IPO structure to pay those guys back, but the main point is that the likely valuation will be in the $1.5-2.5bn range.
But there’s another problem. And it’s one I have some personal experience with. I must stress that my experience is not with Hinge.
As it happens I did a video interview at Hinge’s booth at HLTH in 2022 when my back collapsed, and I got to try out their Enso device (it helped a bit but not much after the first few minutes using it). I discussed the process with PT Lori Walter and got a quick interview with President Jim Pursely (an old Livongo hand BTW).
But this past summer I used the services of their main competitor, Sword Health. As far as I can tell the two companies are very similar in their process and services, both with self-service exercises delivered via the smartphone and both moving from remote care from therapists to AI therapists. But I could be wrong. So for this article I am extrapolating from one company to the other to look at the field of MSK digital services overall.
In total, I thought the Sword experience was good as a standalone program. But the problem was that it was standalone.
My problem was with my left knee. I had a lot of knee surgery in 2002-4 as the result of snowboarding into a tree (Hint. If you snowboard, try to make sure you and the board go the same side of the tree). More than 20 years later in 2024 I managed somehow to induce terrible pain in the knee running for a ferry in January, a train in May and an airport shuttle in June. (It seems that travel and my knee disagree). This didn’t stop me strapping up, taking drugs and snowboarding in the 2024 winter season but it certainly slowed me down a whole lot. Around this time there were many reports of people much younger than me getting their knees replaced.
So I thought I should do something about it. My Blue Shield of California plan offers Solera which is an agglomeration marketplace of digital health apps and services. Sword Health is their PT app, so I selected it, enrolled and off I went.
Note that there was zero integration with my PCP, any orthopedic surgeon, any clinical person at the health plan or basically anyone. This was purely patient-driven and managed.
With Sword I had a 15 min intro call on June 6 – then was sent a box containing a generic tablet and six sensors which fit into straps that you attach to your lower and upper legs and arms.
There was a conversation in the app with a PT and then it spat out a selection of exercises for me. The example below is my second exercise session. If you want to check out more, I have put more of the exercise and the chat with the PT here.
Sword suggested, instead of regular 45-60 minute physical PT sessions, that I did four 15 minutes sessions a week. Essentially one every other day.

The end result was that I did eight sessions between June 12 & June 30.
Continue reading…