More tales of the woes of dealing with health insurance. I live in Marin County, California and one of the things that comes with that is a diagnosis of ADHD for my children. (OK, I have made that joke before but it is true!). My kids now visit a psychiatrist for more sophisticated med management than they receive at their pediatrician. We were (until recently) on a Blue Shield HMO via the Covered California exchange.
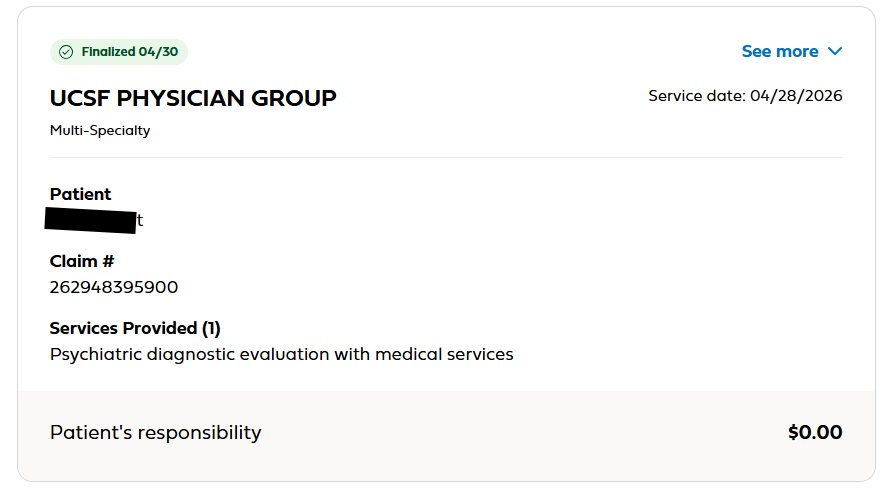
While I was at the doctor’s office, I talked to the staff. They told me I owed a $50 copay. I didn’t pay them (yet) and I went online and saw the claim
The reasonable, informed consumer might think that I owed nothing. The clue being that “Patient Responsibility” was $0.
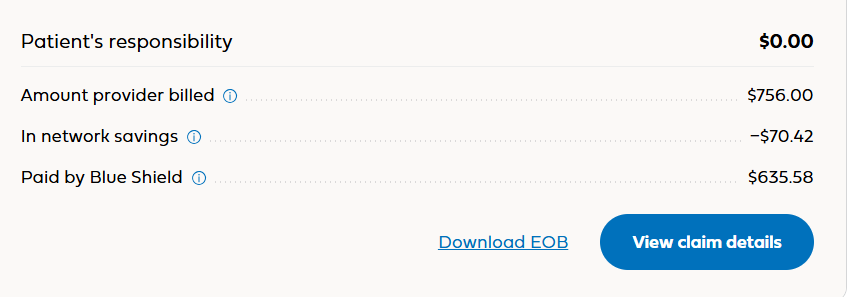
But if you click the “See More” in the top right it shows you this
You probably still think that I owe $0. But if you add the numbers on the right you might notice they don’t total $0.
Until a couple of days ago I hadn’t heard of the phrase “meat computer.” Apparently this has been around for some time, and, as Lora Kelley discusses in The New York Times, the tech elites are increasingly using it, either as a way to humanize AI or as a way to disparage what humans can do relative to AI (e.g., Elon Musk posted last summer, “We are all dumb meat computers compared to digital superintelligence.”).
Raphaël Millière, an associate professor at the University of Oxford, told Ms. Kelley that the metaphor aims to“move the public perception on how humanlike and intelligent frontier models are.”
Encyclicals are, it appears, one of the highest forms of teaching that a pope can give, and it is rare for a pope to deliver one himself, so this is something he takes very seriously. As he should.
AI, he asserts, is the new industrial revolution, and he calls for us to “disarm” it: “Disarming AI means freeing it from the mentality of ‘armed’ competition, which today is not limited simply to the military context, but is also an economic and cognitive phenomenon. Disarming does not mean renouncing technology, but preventing it from dominating humanity.”
“Artificial intelligence needs to be disarmed, freed from the logic that turned it into an instrument of domination, exclusion and death,” he said. “It must be at the service of all, and of the common good.”
The pope makes it clear that he is not against technology per se – “technology should not be considered, in itself, as a force antagonistic to humanity” – but the question is how it is used and what the impact on people will be. “For this reason, merely regulating it is insufficient; it must be disarmed, welcoming and accessible,” he said.
He is particularly concerned about control over AI, and the wealth that comes from it, should not be concentrated among an elite few:
Call 988 in California and someone picks up. In parts of the state, a mobile crisis team might arrive at your door instead of police. Through Proposition 1, the state is putting billions into treatment beds, supportive housing, and youth services. On paper, California is in the middle of the most ambitious behavioral health expansion in the country.
Even as demand for mental health and substance use treatment surges, the supply of trained professionals is not keeping pace. California needs 375,000 behavioral workers by 2030, doubling positions statewide. State officials estimate a 38% shortfall in psychiatrists and a gap of roughly one-third among the 100,000 licensed therapists needed. Rural and underserved communities are especially hard hit; many have no child and adolescent psychiatrists at all. And shortages extend beyond doctors and therapists. Clinical social workers, addiction counselors, peer support specialists, and community health workers are also in short supply.
Building on State Leadership
California is not starting from scratch. The Department of Health Care Access and Information (HCAI) already administers several scholarship and loan repayment programs that encourage clinicians to practice in high-need settings, including loan repayment for nurses, licensed mental health providers, substance use disorder counselors, and psychiatric nurse practitioners. Through the BH-CONNECT federal waiver, HCAI is rolling out five workforce programs over 2025–2030, including a Medi-Cal Behavioral Health Student Loan Repayment Program.
These are important efforts, but they aren’t scaled to the size of the crisis. Loan repayment awards are often a fraction of a graduate’s full debt, and have limited availability. Even the largest programs will only target a few hundred providers; California needs thousands more.
Repayment alone doesn’t solve the immediate affordability problem: people can’t enter training if they can’t pay rent while they are doing it.
A $1 Billion Statewide Workforce Fund for California
California should create a statewide Behavioral Health Workforce “Pay It Forward” Fund: a $1 billion pool that lends money to trainees at zero interest, gets paid back as they get good jobs, and lends those same dollars out again.
MIT is, most people would admit, a pretty good school. Even those who don’t know a lot about universities probably associate MIT with science, engineering, and math, and in fact, it is one of the leading universities in the world for those (and other) areas. E.g., the QS World University Rankings have named it the top university in the world the last 14 years, USN&WR Global Universities Ranking has it #2, as does The Times Higher Education World University Rankings. There have been over 100 Nobel Laureate recipients associated with MIT. If you meet a Harvard grad you might think, oh, they may not actually be all that smart – they could be just a legacy admission, but if you meet an MIT grad you probably do expect that they must be smart, especially since MIT does not have legacy admissions. Even President Trump, who rails against “elite universities” and who has slashed science funding in his second administration (more on that later), can’t help but rave about his smart uncle who taught at MIT.
So when the President of MIT warns about reductions in research funding and in graduate school admissions, we’re not talking about the proverbial canaries in the coal mine dying. We’re talking about miners going down.
In a video message last week, MIT President Sally Kornbluth warned of some startling losses: over 20% drops in federally funded research, in new federal research awards, and in graduate student enrollment. Overall, the school’s research enterprise has shrunk 10% in the last year.
Gulp.
“That is a striking loss for one of the most influential and productive research communities in the world,“ Dr. Kornbluth said. She added:
The fact is that we’re looking at a real drop in research being done by the people of MIT. It’s a loss of momentum for faculty and students and frankly, it’s a loss for the nation. When you shrink the pipeline of basic discovery research, you choke off the flow of future solutions, innovations, and cures, and you shrink the supply of future scientists.
Make no mistake: although MIT itself may be an outlier, what is happening to it is not. Ted Mitchell, president of the American Council on Education, told The Washington Post: “This is the first of many of these kinds of alarms that will be ringing,” Brendan Cantwell, a professor of higher education at Michigan State University, also told WaPo that if MIT is scaling back how it does research, that means universities across the country should be thinking about scaling back and adjusting. The ripple effects will go far and wide, and will have bigger impacts than we realize.
For decades, quality in healthcare has been defined on industry terms — not people’s terms. New technology and innovative health plan designs are finally changing that.
People know quality when they see it, and they are definitely not seeing it in healthcare. Fifty-six percent of Americans rate the quality of care as “poor” or “fair,” and 90% believe we’re overpaying for it. Likewise, 80% of employers — collectively the largest purchasers of healthcare in the country — say that higher-quality care is a top priority for their workforce.
And yet, the U.S. healthcare system remains a global leader; a lack of know-how or quality control isn’t the problem. The problem is the wide gap between how the healthcare industry has historically defined quality and how quality is experienced by the people actually receiving and paying for care.
For the past 75 years, healthcare quality has been shaped by a grab bag of federal agencies, accrediting bodies, medical organizations, health insurers, and — more recently — consumer-focused ratings outfits ranging from U.S. News & World Report to Zocdoc. Though many pay lip service to patient experience, none has clearly defined quality — or explained it intuitively enough — to help individuals make smarter healthcare decisions based on their clinical and financial context.
Healthcare needs to move beyond narrow metrics and top doc lists to create a dynamic, value-driven view of quality that consistently connects people to the best care for them, where and when they need it — and ideally, even before they know they need it. Too often, “quality” equates to some numbers on a dashboard, when it needs to be more like a combination of GPS and driver-assist technology: guiding people to their health goals, keeping them in the highest-quality lane, and nudging them if they start to drift.
This was always the vision (for some of us). But we simply haven’t had the right mix of technology and system-wide connectivity to bring it to life. Now we do.
A New York Times interview with Rep. Jake Auchincloss (D – Mass) by Bret Stephens caught my attention. I am somewhat familiar with Mr. Stephens from his various pieces in NYT; he is definitely a conservative, but in the old, pre-MAGA sense where it meant you worried about spending but you didn’t hate people who weren’t like you. Rep. Auchincloss, on the other hand, was unfamiliar to me, but the headline of the interview – The Democrat Who Makes Me Listen – proved apt.
For me, the final line the interview summed everything up. Rep. Auchincloss is a Marine veteran, having served in Afghanistan. Mr. Stephens asked: “Final question. If there is one thing you learned in the Marine Corps which every American should know, what is it?” Rep. Auchincloss’s reply was succinct, to the point, and highly instructive: “Officers eat last.”
“Officers eat last” – wow. That’s a philosophy I can buy into. That’s a credo I hope I can live up to. That’s a slogan for a political movement I could get behind.
Of course, I’m not just talking about literally only Marine officers, and I’m not just talking about eating. I’m sure Rep. Auchincloss intended that it was a life lesson that should be applied broadly. I.e., people in authority should make sure the people they are responsible for get taken care of before they take care of themselves. I don’t think that attitude is solely responsible for the esteemed Marine esprit de corps, but it’s got to be part of it.
The trouble is, we don’t see much of that attitude in the rest of America. When Congress failed to pass a budget and millions of federal workers went without paychecks, they (and their staffs) kept getting paid. When the White House went slashing various budgets, it didn’t eliminate White House jobs.
According to Gallup, only 10% of Americans approve of the job Congress is doing, with 86% disapproving, but they don’t care. They get paid anyway, and most House seats aren’t competitive, so most incumbents are in little danger of getting voted out.
This is one of those “Coming Soon” announcements. I spent the weekend with the wonderful gang from what I affectionately call Camp Claudia Cult, a group of mostly Californian policy wonks led by Claudia Williams, who these days is at the UC Berkeley School of public health. As you may have noticed I’ve been spending much of my time writing and talking about the notion of Concierge Care for All. Most of the group at the Health Collab wants to blow up/burn down the current system and replace it with a primary care-driven system. And there’s lots of discussion and planning on how to do that. But there is so much happening in innovation in primary care that I thought we need a dedicated channel to discuss it.
Since the sunsetting of the THCB gang, I’ve been doing lots of tech interviews, but not many about how care works. So now I will. If you want to get involved or be interviewed, please email me — Matthew Holt
By JULIE EGGINGTON, EKATERINA CLEARY & LEEZA OSIPENKO
When CMS issued its Request for Information under the Comprehensive Regulations to Uncover Suspicious Healthcare (CRUSH) initiative in February, it zeroed in on a long-festering problem: fraud, waste, and abuse in laboratory testing, especially in genetic and molecular diagnostics.
The laboratory industry will respond. And when it does, its arguments will sound polished, familiar, and deeply reassuring. They will also be either disingenuous or unproven.
If policymakers want this effort to succeed, they should be prepared to handle three claims that have long shielded problematic practices from meaningful oversight.
Claim 1: Fraud, waste and abuse is limited to a few bad actors
Expect labs to argue that fraud, waste, and abuse is rare, isolated, and already addressed through enforcement actions. The narrative will feature a handful of egregious cases, presented as outliers in an otherwise trustworthy ecosystem.
But the problem is not a few rotten apples. It is the orchard’s design.
Take “code stacking” for example, in which laboratories bill multiple individual genetic test codes rather than a single panel code, often inflating reimbursement. In one analysis, laboratories used between 1 and 12 billing codes for hereditary cancer panels with the same indications for testing, with estimated average charges ranging from $679 to $8,589 for ostensibly comparable tests. The repetition of these behaviors across companies suggests systemic incentives, not isolated misconduct.
A key driver is opacity. Many laboratory-developed tests (LDTs) are marketed under similar or identical names despite meaningful differences in design, accuracy, and intended use. To a clinician or payer, they appear interchangeable. In reality, they are not.
This naming ambiguity allows lower-quality tests to ride the coattails of better-validated ones, while still commanding reimbursement. Fraud, in this context, is not always a dramatic act. It is often embedded in routine billing.
Claim 2: Precision medicine advanced by genetics is worth the cost due to improved patient outcomes
The second argument will appeal to aspiration. Labs will emphasize that genetic testing is the backbone of precision medicine and therefore a worthwhile investment for CMS, despite the ballooning costs.
But of course, fraud and corruption in health care has been going on forever. Back in 2011 a Florida man was convicted of Medicare fraud to the tune of tens of millions and got a 50 year sentence. Don’t be surprised that Trump commuted his sentence. And that’s just one of thousands and thousands of cases, mostly by providers inventing fake patients to defraud Medicare or Medicaid.
But the ones who get convicted and go to jail are the amateurs.
The venue though may have moved. Risk adjustment in Medicare Advantage has become one of the biggest venues for fraud. The key here is that the DOJ and HHS found that while Medicare Advantage plans were upcoding their patients, and therefore getting paid more for them, they weren’t actually delivering more services.
Protecting Healthcare and Our Democracy: A conversation with Mandy Cohen, Former Director, Centers for Disease Control and Prevention PLUS former NC Governor Roy Cooper & Dr. Donald Berwick, IHI founder/former president