
By OWEN TRIPP
Creating a healthcare experience that builds trust and delivers value to people and purchasers isn’t a quick fix, but it’s the only way to reverse the downward spiral of high costs and poor outcomes
Entrepreneurs like to say the U.S. healthcare system is “broken,” usually right before they explain how they intend to fix it. I have a slightly different diagnosis.
The U.S. healthcare system is the gold standard. Our institutions and enterprises, ranging from 200-year-old academic medical centers to digital health startups, are the clear world leaders in clinical expertise, research, innovation, and technology. Capabilities-wise, the system is far from broken.
What’s broken is trust in the system, because of the glaring gap between what the system is capable of and what it actually delivers. Every day across the country, people drive past world-class hospitals, but then have to wait months for a primary care appointment. They deduct hundreds for healthcare from each paycheck, only to be told at the pharmacy that their prescription isn’t covered. While waiting for a state-of-the-art scan, they’re handed a clipboard and asked to recap their medical history.
This whipsaw experience isn’t due to incompetence or poor infrastructure. It’s the product of the dysfunction between the two biggest players in healthcare: providers and insurers, two entities that have optimized the hell out of their respective businesses, in opposition to one another, and inadvertently at the expense of people.
Historically, hospitals and health systems — including those 200-year-old AMCs — have dedicated themselves fully to improving and saving lives. I’m not saying they’ve lost sight of this, but until recently, margin took a back seat to mission. With industry consolidation and the persistence of the fee-for-service model, however, providers’ hands have been forced to maximize volume of care at the highest possible unit cost, which in turn has become a main driver of the out-of-control cost trend at large.
This push from providers has prompted an equal-and-opposite reaction from insurers. Though the industry has been villainized (rightly, in some cases) for a heavy-handed approach to utilization management and prior authorization, insurers are merely doing what their primary customers — private employers — have hired them to do: manage cost. Insurers have gotten very good at it, not just by limiting care, but also through product innovation that has created more tiers and cost-sharing options for plan sponsors.
Meanwhile, healthcare consumers (people!) have been sidelined amid this tug-of-war. Doctors and hospitals say they’re patient-centered, and insurers say they’re member-centric — but the jargon is a dead giveaway. Each side is focused on their half of the pie, and neither is accountable for the whole person: the person receiving care and paying for care, not to mention navigating everything in between.
It should come as no surprise that trust is falling. Only 56% of Americans trust their health insurer to act in their best interest. Even trust in doctors — the good guys — has plummeted. In a startling reversal from just four years ago, a whopping 76% of people believe hospitals care more about revenue than patient care.
| Loss of Trust in Healthcare Providers | |
Hospitals in the U.S. are mostly focused on… | 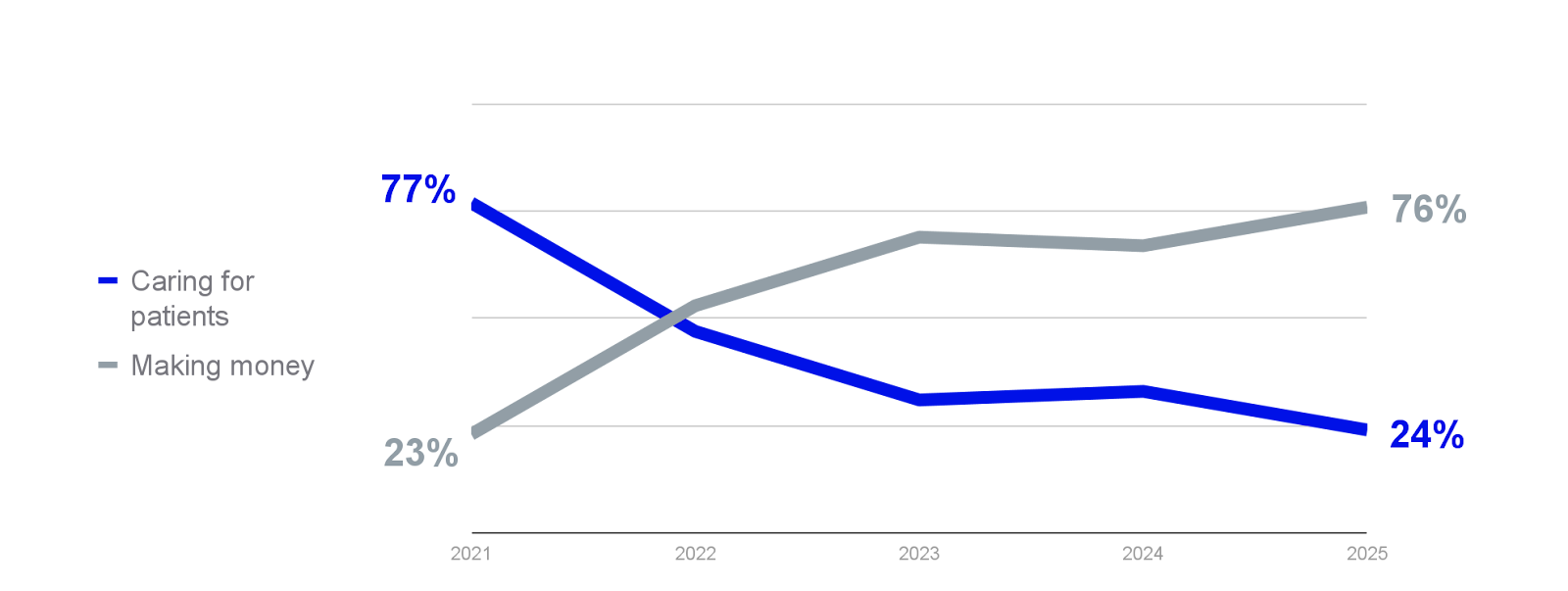 |
| ⏺ Caring for patients⏺ Making money Source: Jarrard/Chartis (2025) | |
This trust deficit is the root cause of so many healthcare problems. It’s the reason people disengage, delay and skip care, and end up in the ER or OR for preventable issues. When a good chunk of the population falls into this cycle, as they have, you end up with the status quo: unrelenting costs and deteriorating outcomes that is dragging down households, businesses, and the industry itself.
There’s no quick fix. Despite what my fellow entrepreneurs might say, no one point solution or technology (no, not even AI) can rebuild trust. The only way to reverse the downward spiral is by serving up a modern experience that is genuinely designed around people’s needs.
Continue reading…















