The United States health care system is a big, expensive mess, and the people working in the system today often don’t even know how to start learning about the system, and it’s problems. My own frustration with the health care system – and lack of teaching about it during medical school – lead me to write The Health Care Handbook: A Clear and Concise Guide to the US Health Care System with my colleague Elisabeth Askin. The goal was to create an understandable primer on the health care system for providers so that we can all work together to improve the system and help our patients.
The United States health care system is a big, expensive mess, and the people working in the system today often don’t even know how to start learning about the system, and it’s problems. My own frustration with the health care system – and lack of teaching about it during medical school – lead me to write The Health Care Handbook: A Clear and Concise Guide to the US Health Care System with my colleague Elisabeth Askin. The goal was to create an understandable primer on the health care system for providers so that we can all work together to improve the system and help our patients.
We have partnered with THCB to provide excerpts from the 2nd edition of the Handbook, which will provide background and insight on important health care issues that we face today. We would love your questions, comments and feedback. Today’s excerpt provides a brief overview of the state of the US health care system today.
Cost
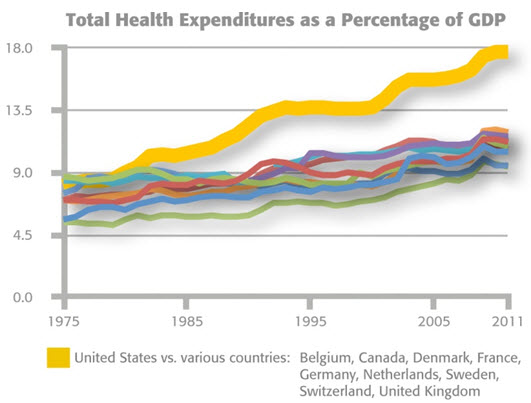
The U.S. currently spends more than 17% of its national gross domestic product (GDP) on health care, far more than any other country in the world. Health care spending now averages almost $9,000 per American,1and health care is the fastest growing industry in the country.2Private (nongovernmental)health care spending accounts for a large portion of the difference between spending in the U.S. and in other industrialized countries.
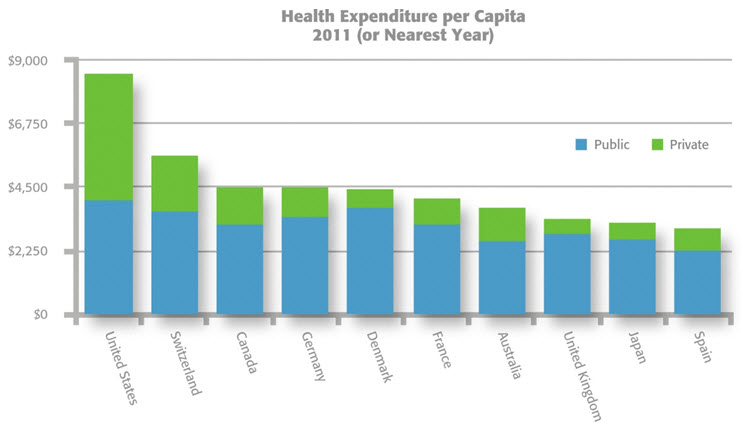 Organisation for Economic Co-operation and Development, “Health Statistics2013,” June 2013. Note: Values in U.S. $ Purchasing Power Parity. Data for Japan and Australia refers to 2008.
Organisation for Economic Co-operation and Development, “Health Statistics2013,” June 2013. Note: Values in U.S. $ Purchasing Power Parity. Data for Japan and Australia refers to 2008.
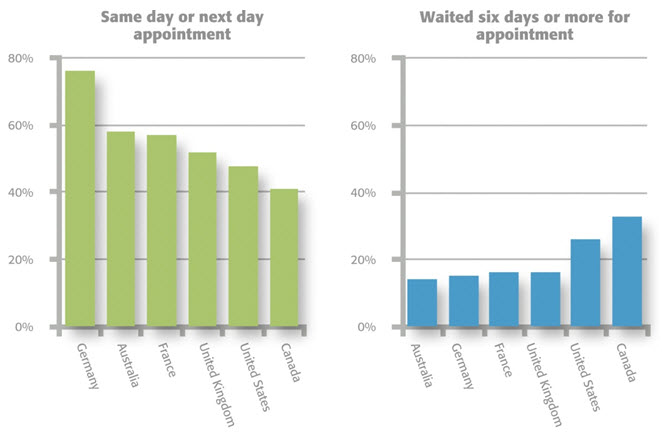
Access
The U.S. has fewer physicians,hospital beds, physician visits,and hospitalizations per capita than most other industrialized countries.3 Eighty-five percent of Americans report having a regular source of ongoing care, but more than a quarter encounter difficulty accessing the healthcare system.4 There are large disparities in access by type of health insurance coverage.