The concept of “centers of excellence” has been around for a few decades. Surely sending health plan members and self-insured employers’ employees to the best and most effective providers should improve health outcomes and save payers’ money? Sach Jain is CEO of Carrum which has been working on this problem, partnering with the best providers and aggregating that demand from employers…and putting it all on a state of the art platform. As you might suspect, it’s not as easy as it looks. Carrum raised $45m from Omers Ventures a few weeks back, on top of a decent raise from Tiger Global a couple of years back. So are they getting it right? Sach told Matthew Holt that they are for sure on their way….
matthew holt
Matthew’s tidbits: Obesity Summer
Every time I get around to sending out the THCB READER I add a short & usually not to sweet commentary on some aspect of health care.–Matthew Holt
I saw the obesity crisis up close this week. And by that I’m not just referring to my addiction to Salted Caramel with Pretzel Ice Cream, bad though it is. Instead I felt thin because I went to Disneyland. But while I tip the scales at a BMI of 30 if I’m lucky, I genuinely felt that looking around Disneyland more than 50% of the crowd were obese and many morbidly so.
The rest of my trip to Southern California was quite a contrast because I’ve been watching a girls water polo tournament. Those young women and most of their families, as you’d expect, look very different. In this crowd I am definitely on the other end of the spectrum.
Obviously there’s a big socio-economic difference between the Disneyland attendees and a crowd centered around a sport largely played by rich, white kids. But at a time where we are arguing about whether Ozempic and its fellow anti-obesity drugs should be available via insurance, we seem to have no other strategies to fight the nation’s slide to obesity.
You’ve probably seen those photos of people on the beach in the 1960s where everyone is thin. I won’t claim to understand the science of what happened but clearly the prevalence of high fructose corn syrup and other highly processed food has much to do with it. As does the free rein food companies have had to advertise what are addictive products. I don’t know how we get to be a nation where everyone eats and exercises like a water polo player. But clearly we need significant changes in our agriculture and nutrition policies. We did it with smoking, so we know it can be done. If you don’t think we need it, I recommend a trip to Disneyland (and that’s the only reason I recommend one!)
Not The Last of Them

By KIM BELLARD
I’m seeing two conflicting yet connected visions about the future. One is when journalist David Wallace-Wells says we might be in for “golden age for medicine,” with CRISPR and mRNA revolutionizing drug development. The second is the dystopian HBO hit “The Last of Us,” in which a fungal infection has turned much of the world’s population into zombie-like creatures.
The conflict is clear but the connection not so much. Mr. Wallace-Wells never mentions fungi in his article, but if we’re going to have a golden age of medicine, or if we want to avoid a global fungal outbreak, we better be paying more attention to mycology – that is, the study of fungi.
We don’t need “The Last of Us” to be worried about fungal outbreaks. The Wall Street Journal reports:
Severe fungal disease used to be a freak occurrence. Now it is a threat to millions of vulnerable Americans, and treatments have been losing efficacy as fungal pathogens develop resistance to standard drugs.
“It’s going to get worse,” Dr. Tom Chiller, head of the fungal-disease branch of the Centers for Disease Control and Prevention, warns WSJ.
A new study found that a common yet extremely drug resistant type of fungus — Aspergillus fumigatus – has been found even in a very remote, sparsely populated part of China. Professor Jianping Xu, one of the authors, points out: “This fungus is highly ubiquitous — it’s around us all the time. We all inhale hundreds of spores of this species every day.”
We shouldn’t be surprised, because fungi tend to spread by spores In fact, according to Merlin Sheldrake’s fascinating Entangled Life: How Fungi Make Our Worlds, Change Our Minds, and Shape Our Futures, fungi spores are the largest source of living particles in the air. They’re also in the ground, in the water, and in us. They’re everywhere.
That sounds scary, but without fungi, we not only wouldn’t be alive, we never would have evolved.
Continue reading…Matthew’s health care tidbits: Time to get Cynical
Each time I send out the THCB Reader, our newsletter that summarizes the best of THCB (Sign up here!) I include a brief tidbits section. Then I had the brainwave to add them to the blog. They’re short and usually not too sweet! –Matthew Holt
Plenty of reason to worry about the future of American health care this week. The biggest for-profit hospital chain–HCA–was accused of aggressively pushing patients into hospice care, sometimes in the same room, in order to make their hospitality mortality numbers look better. Most of the leading benefits consulting companies were exposed as taking payments from PBMs–yup, the same organizations their employer clients thought they were negotiating with on their behalf. And one of the biggest names in digital health, Babylon Health, tumbled into destitution, taking billions of dollars with it and leaving uncertain the fate of the medical groups in California it bought less than two years ago. Even the most successful capitalists in health care — United HealthGroup and its fellow insurers — saw their stock fall because apparently outpatient surgery volume is ticking up.
On the policy front the malaise is spreading too. The end of the public health emergency (remember Covid?) is being used as an excuse by the old confederate states to kick people off Medicaid. Georgia and Arkansas appear to be bringing back work requirements, even though I thought CMS has banned them and every study has acknowledged that they are cruel and ineffective. About 20 million people got on to Medicaid during the public health emergency and KFF estimates up to 17 million may be kicked off, while over 1.7 million already have.
Finally an article by Bob Kocher and Bob Wachter in Health Affairs Scholar remins us that big academic medical centers are nowhere near ready for value-based care (VBC). Jeff Goldsmith has been vocal on THCBGang and elsewhere about how VBC is becoming a religion more than a reality. And I remind you that Humana’s MA program is still basically a Fee-For-service program in drag (even though that’s now illegal in their home state).
I grew up in American health care expecting that eventually a combination of universal insurance mixed with value-based purchasing would lead to a series of tech-enabled companies doing the right thing by patients and making money to boot. With the managed care revolution, the ACA and the boom in digital health all firmly in the rear view mirror, the summer of 2023 is a lesson that you can never be too cynical about health care in America.
.
As Health Professionals Go, So Goes Our Democracy
By MIKE MAGEE
Last weekend’s New York Times headline, The Moral Crisis of America’s Doctors, spotlights that there is growing concern that the monetarization and corporatization of nursing and medical professions by hospital and insurance power houses, have seriously undermined the mental health and ethical effectiveness of health care professionals. The pandemic has only heightened the crisis.
Since focusing on the social science of Medicine in the 1990’s in Philadelphia, it has been an uphill battle to convince leaders in and out of Medicine that doctors and nurses are critical to individual and societal success. Recently, I’ve come to the conclusion that this may have more to do with a general lack of knowledge of our form of governing, democracy, than a misunderstanding of the stabilizing effect of professional doctors and nurses.
What is democracy? For an answer I turned to John J. Patrick PhD, professor emeritus in history, civics and government at the Indiana University. In his “Understanding Democracy,” he explains that democracy as we know it is a “startling new development.” The practice of rule (krater) by the people (demos), or “demokratia,” dates back 2500 years to Athens, Greece. Citizens did rule by majority vote, but only free males of Greek descent could rise to the status of “citizen.” In those days, individual freedoms took a back seat to unconditional support of the city-community.
Establishing a modern democracy in America has been a bit of a struggle.
Continue reading…Interview with Dr Pamela Tenaerts, Medable
Pam Tenaerts is the Chief Scientific Officer of Medable, which went from being a small company creating software helping clinical researchers to design their own experiments to being the big dog in remote clinical trials during the pandemic. Medable has raised over $500m in the past 3 years. Pam has a stellar research background and this interview covers the gamut about how clinical trials work, which companies are involved, how remote (or hybrid) trials actually work, and what the likely outcome for clinical research will be. If you have any interest in understanding the state of play in pharma R&D, this is compulsory viewing–Matthew Holt
Matthew’s health care tidbits: Hedge Funds that Do Health Care on the Side
Each time I send out the THCB Reader, our newsletter that summarizes the best of THCB (Sign up here!) I include a brief tidbits section. Then I had the brainwave to add them to the blog. They’re short and usually not too sweet! –Matthew Holt
Lots of news about bad behavior in health care this week, with real shots about patient & staff safety at home care company Papa, and Grail misinforming 400 people that they had cancer. But the prize for tone deafness this week comes from another very well funded health care provider system being heartless to its poorest patients.
This week it’s Allina, a Minnesota “nice” system which actually amended its Epic system so that clinicians could literally not book appointments or provide care to patients who owed Allina money. Clinicians on the sharp end of this were so appalled that they went on the record about their own employer to NY Times’ reporter Sarah Kliff. The most egregious example was a doctor unable to write a prescription for a kid that had scabies–an infectious parasitic disease–who was sharing one bed with two other kids!
Of course Allina also is on the low end of charity care provision (below 1% of revenues). In contrast ten employees make more than $1m a year and another 10 make more than $500,000.
We all know about egregious private equity funds investing in payday loans and other scummy outfits that prey on the poor. Turns out that if you let a non-profit hospital become beholden to its financial, rather than moral, north star, it starts to behave in a similar manner. Allina, of course, had a smidge under $4bn in its “investment reserve” at the end of 2021. It’s by no means special. UPMC has over $7bn in its reserves (unclear if this includes the investments it has made in startups), while Ascension has a formal private equity fund that controversially paid its former CEOs over $10m as part of its $18bn reserves.
Somehow having hedge funds that provide a little health care service on the side doesn’t leave the best taste in the mouth for how we should be organizing this health care system.
What Can We Learn from the Envision Bankruptcy?

By JEFF GOLDSMITH
Envision, a $10 billion physician and ambulatory surgery firm owned by private equity giant Kohlberg Kravis Roberts, filed Chapter 11 bankruptcy on May 15. It was the largest healthcare bankruptcy in US history. Envision claimed to employ 25 thousand clinicians- emergency physicians, anesthesiologists, hospitalists, intensivists, and advanced practice nurses and contracted with 780 hospitals. Envision’s ER physicians delivered 12 million visits in 2021, not quite 10% of the US total hospital ED visits.
The Envision bankruptcy eclipsed by nearly four-fold in current dollars the Allegheny Health Education and Research Foundation (AHERF) bankruptcy in the late 1990’s. KKR has written off $3.5 billion in equity in Envision. Envision’s most valuable asset, AmSurg and its 257 ambulatory surgical facilities, was separated from the company with a sustainable debt structure. And at least $5.6 billion of the remaining Envision debt will be converted to equity at the barrel of a gun, at dimes on the dollar of face value.
KKR took Envision private in 2018 when Envision generated $1 billion in profit, in luminous retrospect the peak of the company’s good fortune. Envision’s core business was physician staffing of hospital emergency departments and operating suites. In 2016, then publicly traded, Envision merged with then publicly traded ambulatory surgical operator AmSurg. This merger seemed at the time to be a sensible diversification of Envision’s “hospital contractor” business risk.
Indeed, Envision’s bonus acquisition of anesthesia staffing provider Sheridan, acquired by AMSURG in 2014, helped broaden its portfolio away from the Medicaid intensive core emergency room staffing business (EmCare), which required extensive cost-shifting (and out of network billing) to cover losses from treating Medicaid and uninsured patients. It is clear from hindsight that where you start, e.g. your core business, limits your capacity to spread or effectively manage your business risk, an issue to which we will return.
The COVID hospital cataclysm can certainly be seen as a proximate cause of Envision’s demise.
The interruptions of elective care and the flooding of emergency departments with elderly COVID patients, which kept non-COVID emergencies away, damaged Envision’s core business as well as nuking ambulatory surgery. By the spring of 2020, Envision was exploring a bankruptcy filing. An estimated $275 million in CARES Act relief and draining a $300 million emergency credit line from troubled European banker Credit Suisse temporarily staunched the bleeding. But the pan-healthcare post-COVID labor cost surge also raised nursing expenses and led to selective further shutdowns in elective care and further cash flow challenges.
While one cannot fault KKR’s due diligence team for missing a global infectious disease pandemic, with hindsight’s radiant clarity, there were other issues simmering on the back burner by the time of the 2018 deal that should have raised concerns. Two large struggling investor owned hospital chains, Tenet and Community Health Systems, began divesting marginal properties in earnest in 2018, placing a lot of Envision’s contracts in the pivotal states of Florida and Texas at risk.
More importantly, there were escalating contract issues with UnitedHealth, one of Envision’s biggest payers, as well as increasing political agitation about out-of-network billing, which provided Envision vital incremental cash flow. These problems culminated in a United decision in January 2021 to terminate insurance coverage with Envision, making its entire vast physician group “out of network”.
Continue reading…SPM-Creative Learning Exchange, Portland, OR (& virtual), July 16

As you may know I am on the board of the Society for Participatory Medicine (SPM) which is trying to promote a new partnership between patients and the health care system.
On June 16 at 8am-1pm PST SPM is hosting a Creative Learning Exchange in Portland, OR at OHSU. The topic is Advancing Health Equity Through Participatory Medicine and there’ll be patients, clinicians and other leading crucial discussions about how to move health equity forward.
If you are in Portland please come join the meeting and if you can’t get there, it will be broadcast online. (There’s a nominal cost for tickets but no one will be turned away if they can’t afford it) Click here to find out more.–Matthew Holt
Healthcare Data: The Disruption Opportunity + Why This Time Is Different
By SHUBHRA JAIN & JAY SANTORO


Knowledge is power. If this adage is true, then the currency of power in the modern world is data. If you look at the evolution of the consumer economy over the past 100 years, you will see a story of data infrastructure adoption, data generation, and then subsequent data monetization. This history is well told by Professors Minna Lami and Mika Pantzar in their paper on ‘The Data Economy’: “Current ‘data citizenship’ is a product of the Internet, social media, and digital devices and the data created in the digitalized life of consumers has become the prime source of economic value formation. The database is the factory of the future.” If we look no further than the so-called big tech companies and distill their business models down in a (likely overly) reductionist fashion: Apple and Microsoft provide infrastructure to get you online, and Facebook (Meta) and Google collect your data, while providing a service you like, and use that data to sell you stuff. Likely none of this is surprising to this audience, but what is surprising is that this playbook has taken so long to run its course in one of the world’s largest and most important sectors: healthcare.
Given the potential impact data access and enablement could have on transforming such a large piece of the economy, the magnitude of the opportunity here is — at face value — fascinating. That said, healthcare is a different beast from many other verticals. Serious questions arise as to whether target venture returns can be extracted in this burgeoning market with the scaled incumbents (both within and outside healthcare) circling the perimeter. Additionally, this is a fragmented ecosystem that has existed (in its infancy) for a few years now with well-funded players now solving for different use cases. Thus, another question emerges as to which areas are best suited for upstarts to capitalize. A key theme in our assessment of the space is that regulation is driving the move towards democratized data access in healthcare, but unlike in regulatory shake-ups of the past, this time start-ups will benefit more than scaled incumbents. Furthermore, we have identified some areas within each approach to this new ecosystem that particularly excite us for net new investment. Let’s dive in.
Why This Time is Different: Regulatory + Market Dynamics
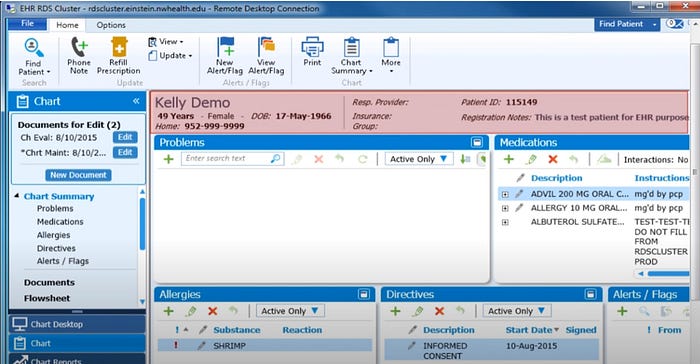
The Health Information Technology for Economic and Clinical Health (HITECH) Act of 2009 brought about an explosion of digital healthcare data by expanding adoption of electronic medical records from ~12% to 96%.