


By PHUOC LE MD, CONNIE CHAN and BROOKE WARREN
Since the World Health Organization (WHO) officially declared COVID-19 a pandemic on March 11, 2020, we have been changing our daily lives to protect the highest-risk populations: older adults and people with chronic medical conditions. We are asked to follow sensible guidelines like social distancing and thorough hand-washing. Although one may have a gut-reaction to put their own safety at the forefront during these times of crisis, it is essential that we are taking the necessary steps to protect populations with additional vulnerabilities – rural tribal communities.
With the announcement that COVID-19 reached the Confederated Tribes of Umatilla Indian Confederation on March 9, 2020, it was evident the virus would not stay confined to urban and metropolitan centers like some previously predicted. The experience in China with COVID-19 clearly reflects the vulnerability of rural communities because many people travel routinely from urban to rural. Experts who conducted an epidemiological study in Hubei province, the initial epicenter of the COVID-19 pandemic, noted in their report: “…most public medical resources are concentrated in cities but are relatively scarce in rural areas. Therefore, prevention and treatment of 2019-nCoV in rural areas will be more challenging if new phases of the epidemic emerge.”

Dalee Sambo Dorough, Ph.D. (Inupiaq) reminds us that American Indian/Alaskan Native (AIAN) people have “had a whole history of epidemics that have devastated [their] communities in the past.” These historical traumas are compounded by the reality that more AIAN people have underlying health conditions, putting them at even greater risk for morbidity and mortality due to COVID-19. For example, in 2010, the Indian Health Service released a report that showed AIAN individuals were 1.5 times more likely to have renal disease, 3.2 times more likely to have diabetes mellitus and 4.6 times more likely to have chronic liver disease compared to all other U.S. racial categories. These are all conditions that are known risk factors for complications and death due to COVID-19.
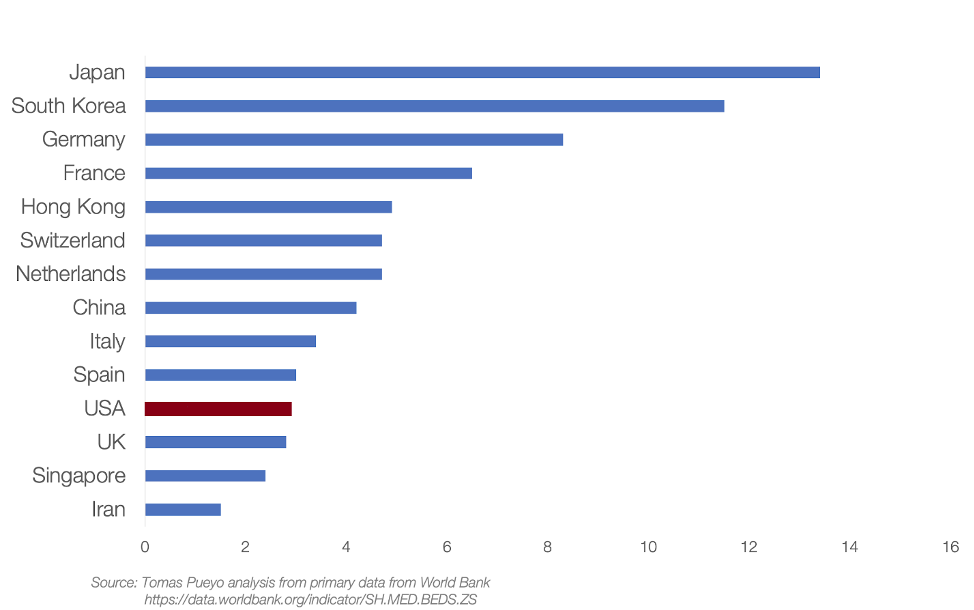
Exacerbating this reality is the fact that access to health care in rural areas in the U.S. is still widely inadequate. Rural hospitals and clinics are already overburdened at baseline. Pertinent to COVID-19 is the extremely low number inpatient and ICU beds and ventilators available in rural settings, making it likely that COVID-19 patients will suffer delays in care (see Figure 1 below). COVID-19 is therefore an acute on chronic crisis. This will widen the existing inequalities that are already prevalent between urban and rural care when it comes to accessing essential resources and priority. One ER provider working in a rural hospital notes, “Even a small number of patients showing up in the emergency room all at once could quickly overwhelm tiny rural hospitals. Testing isn’t as simple as running a swab over to a nearby public health lab — a courier has to pick up the samples once a day and drive them hundreds of miles. And if a doctor is accidentally exposed to a patient who tests positive for coronavirus? That could be the one doctor the hospital had.”
Even though federal legislation was recently passed to expand telemedicine in outbreak areas, telemedicine availability is still limited for rural residents. As of 2018, about one-fourth of rural Americans lack access to high-speed Internet. Furthermore, limited access to the Internet further prevents rural residents from working from home to avoid coming into contact with those who are infected.
As we attend to patients and prepare for the spread of COVID-19 into rural areas, we as healthcare workers need to be cognizant of the structural inequalities at play and how they might change the treatment plans we write for our patients. Moreover, we must coordinate with communities to minimize exposure – taking into account living situations, access to clean water, Internet availability, and preexisting conditions of rural communities. One’s location, identity, and circumstance should not dictate the quality of care we provide even when the system is stretched thin during this crisis. We must take the opportunity to provide even more compassionate care and do our best to minimize the inequalities that pervade our healthcare system.
Internist, Pediatrician, and Associate Professor at UCSF, Dr. Le is also the co-founder of two health equity organizations, the HEAL Initiative and Arc Health.
Connie Chan and Brooke Warren are interns at Arc Health who studied Economics and Public Health, and Native American Studies, respectively.
This post originally appeared on Arc Health here.
Categories: Uncategorized







