 On November 15, 2017, an epidemic of hypertension broke out and could rapidly affect tens of millions of Americans. The epicenter of the outbreak was traced back to the meeting of the American Heart Association in Anaheim, CA.
On November 15, 2017, an epidemic of hypertension broke out and could rapidly affect tens of millions of Americans. The epicenter of the outbreak was traced back to the meeting of the American Heart Association in Anaheim, CA.
The pathogen was released in a special 488-page document labeled “Hypertension Guidelines.” The document’s suspicious content was apparently noted by meeting personnel, but initial attempts to contain it with an embargo failed and the virus was leaked to the press. Within minutes, the entire healthcare ecosystem was contaminated.
At this point, strong measures are necessary to stem the epidemic. Everyone is advised not to click on any document or any link connected to this virus. Instead, we are offering the following code that will serve both as a decoy and as an antidote for the virulent trojan horse.
Only a strong dose of common sense packed in a few lines of text can possibly save us from an otherwise lethal epidemic of nonsense. Please save the following text on your EHR cloud or hard-drive, commit it to memory or to a dot phrase, and copy and paste it on all relevant quality and pay-for-performance reports you are asked to submit.
PREAMBLE:
- The blood pressure is a physiologic quantity necessary for, and indicative of, human life.
- The blood pressure normally fluctuates for moment to moment. The range of values encompassed by the blood pressure is wide and depends on personal characteristics, as well as circumstances. For example, during sleep, invasively measured systolic blood pressure in healthy individuals may fall to 70 mmHg or even lower. During weightlifting, the systolic blood pressure may rise as high as 480/350 mmHg.
- Pitfalls that can potentially limit the accuracy of the measurement of blood pressure are many.
- The so-called “resting” blood pressure measured in asymptomatic individuals has statistical significance regarding the long-term health of the individual: the resting blood pressure relates to a risk of adverse health outcomes. That risk is estimated by large scale clinical studies and is modified by patient circumstances.
- The statistical relationship between the resting blood pressure and health is J-shaped.
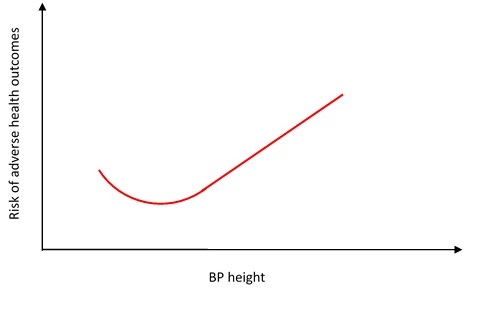
- Because the relationship between blood pressure height and outcomes is statistical, the nadir of the J-shaped curve cannot be determined on an individual basis.
- Because the nadir of the curve cannot be determined on an individual basis, and because the relationship between the blood pressure height and risk is continuous and gradual, no specific blood pressure value or range of values can segregate “normal” from “abnormal” blood pressure.
- In the 1950s Sir George Pickering described any selection of normal values as “the fallacy of the dividing line.” It was a fallacy then, it remains a fallacy now.
HYPERTENSION GUIDELINE:
- Doctors are called to act prudently and to take into account individual patient circumstances that may impact on diagnosis and treatment (Recommendation Class: I; Level of Evidence: C).
- The guideline for the treatment of high blood pressure is to understand the above graph (Recommendation Class: I; Level of Evidence: C).
Categories: Uncategorized








Hypertension is the curse of Modernization. More and more will die of hypertension in this Industrialized society.
Is it safe to exercise for high blood pressure?
http://healthyfit07.blogspot.in/2017/06/exercise-for-high-blood.html
Indeed this seems like disease-state creep, as we have seen with statins. Importantly, not only is the accurate measure of BP difficult and sketchy but so is quantification of long term benefit. That said, it does not like seem bad public health policy to get docs super focused on nudging lifestyle changes for people in the marginal HBP category (after multiple measures)
I wonder if there might be a biologic marker for excess-too-high-blood-pressure over time?… akin to HgbA1c? for the time integral of glucose?
E.g. maybe schistocytes are produced by the shearing stress of hypertension? Of course, these are absent–or extremely rare–in normal blood films where DIC and mechanical trauma by fibrin strands to the red cells are absent. But maybe in hypertension there might be a few more of these in say one thousand or ten thousand red cells?
Or maybe in hypertension there might be a trace of free hemoglobin in the plasma, much less than we usually measure, but present in microgram amounts?
Once again pointing out that medicine is an art as well as a science and measuring pure numbers is not the way to determine quality.
I predict this will be a “performance measure” soon and much like trying to reduce readmissions was correlated with increased mortality, this focus on a number is going to lead to falls, syncope etc.
No matter the messy measurement techniques and disagreements, etc., there is probably some truth buried in the notion that a little increase in resting blood pressure results in a little increase in morbidity–dbp/dt=dm….a little change in blood pressure over time leads to a little increase in morbidity.
After all, we don’t want an essential biological engine to have to put out more energy than it needs to.
We just need to sharpen up our science and data in this effort to clarify.
“Because the relationship between blood pressure height and outcomes is statistical, the nadir of the J-shaped curve cannot be determined on an individual basis.
Because the nadir of the curve cannot be determined on an individual basis, and because the relationship between the blood pressure height and risk is continuous and gradual, no specific blood pressure value or range of values can segregate “normal” from “abnormal” blood pressure.”
Something we teach medical students (at least I do) about BP and any number of other problems. What is your solution? Trying to apply large scale statistical studies to individual patients is part of what we need to do. How do you propose we apply this on an individual basis, remembering that we not only have individual variability in our patients but also with our clinicians.
Steve
I first try to judge if the apparent elevation in BP is real or not, sustained or not, etc. I say “judge” because in itself it’s a decision. The decision is not triggered by the numbers. Depending on the patient or context, the judgment can come quickly or can take a long time. So I also have to make a judgment as to whether there is any urgency to make the decision. The factors that enter into that decision are innumerable. If need be, and if appropriate, I may also use some tests (is there early end organ effect? One of the link above is to a paper I wrote about that). Also factored in is the patient’s attitude toward treatment, risk tolerance, insight, etc…When you factor in all this, the question of cut-off numbers makes no sense. What you deal with is a general sense that the blood pressure may need attention. I suspect it would be ideal for anyone to have a BP<120/80. But that doesn't mean that everyone who's not at ideal BP needs a protocol triggered by a number.
If you knew me, you would know that’s the furthest thing from my mind. I see neither of those terms as euphemisms.
I will try it again, however. What is your approach to starting BP therapy?
I ignore this as I ignore the cholesterol panic. With the ACA going away preexist exclusions for BP will put insurance more out of reach for those not subsidized by employment or Medicare/Medicaid. The drug companies are basking in their stock options.
Risk stratify? Treatment threshold? Brad, your managed care lingo triggers me! 🙂
I already have DOT truckers obsessing about the 140/90 threshold. They are going to really go nuts now.
The first step requires a facility defined process for the conditions and technique required for a standard BP, e.g., fully extended right arm that is supported on a flat surface. A training process is maintained for all new employees and periodically thereafter. The person’s medical record includes a means to track each blood pressure result by date, especially for Routine Health Maintenance visits and separately for each visit, if taking more than 1-2 medications daily (no matter who prescribes them). For an initial result that falls out side of known results, the provider should repeat the blood pressure themselves. Primary Healthcare is not possible in the long run, if there is no flowsheet for Health Maintenance and separately for chronic illness surveillance.
.
Then it becomes really complicated, especially if the baseline measurement process is not standardized for all the personnel in a clinic, such as the technique and criteria for assessing diastolic Blood pressure. In addition, the availability of alternate cuff sizes must assured at the location used to take a blood pressure. The frequency of visits for falsely high blood pressure are common and should be taken seriously because they can eventually evolve into sustained high blood pressure. Equally, there is a tendency to either not measure a blood pressure at all or do it poorly in non-over weight young adult males, especially if they have very infrequent visits. Periodic chart audits are appropriate for Primary Healthcare for this problem.
.
almost…Time to stop. Its much easier to control high blood pressure with an early start, even without medication, and a future trial off becomes an easier alternative with a stable starting point. The most important complication to prevent is an acute MI in the middle of the night. Thus, the initial med for a non-diabetic should be low-dose atenolol at bedtime. Everything else is circumstance driven. DONE
How do you risk stratify folks in your own practice and what is your treatment threshold trigger?