 The idea that payment should be linked to the value lies at the heart of most of the transactions we participate in on a daily basis. Yet, value based payment in healthcare has seemingly run into very rocky waters as of late. It is at this precarious time that stakeholders representing large employers and other purchasers of health care’ took to the Harvard Business Review to write in defense of value based payment reform. The authors pepper their article with cherry picked ‘successes’ of the value movement and urge the country to forge ahead on the current path. The picture that comes to my mind hearing this is of the Titanic, forging ahead in dark waters, never mind the warning signs that abound.
The idea that payment should be linked to the value lies at the heart of most of the transactions we participate in on a daily basis. Yet, value based payment in healthcare has seemingly run into very rocky waters as of late. It is at this precarious time that stakeholders representing large employers and other purchasers of health care’ took to the Harvard Business Review to write in defense of value based payment reform. The authors pepper their article with cherry picked ‘successes’ of the value movement and urge the country to forge ahead on the current path. The picture that comes to my mind hearing this is of the Titanic, forging ahead in dark waters, never mind the warning signs that abound.
One of the authors of the paper – Leah Binder – is President and CEO of the Leapfrog Group – a nonprofit organization founded in 2000 dedicated to triggering ” giant leaps forward in the safety, quality and affordability of U.S. health care by using transparency to support informed health care decisions and promote high-value care”. This is a laudable goal, but it is very much predicated on the ability to measure value. A perusal of the Leapfrog group’s homepage notes a 1000 people will die today of a preventable hospital error.
The warning is explicit – choosing the hospital you go to could be the difference between life or death. I have spent some time in the past about the remarkably weak data that lead to an estimate of 400,000 patients dying per year in hospitals due to medical errors, but suffice it to say the leapfrog group subscribes to the theory that of the ~700,000 deaths that happen in hospitals per year, half are iatrogenic. With no exaggeration, I can say firmly that those who believe this are in the same company as those who believe the earth is flat. If the home page of the Leapfrog group, examination of their claims in their HBR article merits additional concern.
The first example proferred relates to a reduction in venous thromboembolism or blood clots acquired in hospitals after a government agency (AHRQ) began tracking this from 28,000 in 2010 to 16,000 in 2014. Binder et al., note that this means 12,000 fewer patients had ‘potentially fatal blood clots’. Ostensibly this reduction in clots was due to reporting of these events and a Bush era rule from 2008 that put hospitals on notice that Medicare would no longer be paying for Hospital acquired Conditions (HAC) like clots after joint surgery. But how exactly did hospitals achieve these impressive results? While the hope is that hospitals achieved these reduction by better attention to therapies that prevent blood clots, the reality is somewhat more complicated.
For starters, orthopedic surgeons grew wary of searching for blood clots postoperatively. The surgeons weren’t necessarily wrong to adopt a newly parsimonious approach. Easy access to ultrasounds and cat scans meant many patients ended up diagnosed with small clots in the calf or in the small arteries of the lung that were unlikely to cause the patient harm. It was not lost on surgeons that these clots were unlikely to be fatal to the patient, but were potentially fatal to the hospital and surgeon’s bottom line.
Yet another way of reducing hospital acquired conditions is to improve the diagnosis of blood clots that patients carry with them on admission. It is clearly unfair to penalize hospitals for patients who present with a blood clot, so improving the diagnosis of these patients is important. Unfortunately, too much of a good thing is usually too much of a good thing. Some institutions actually began performing screening whole leg ultrasounds on all inpatients being admitted. The whole leg is important because asymptomatic blood clots that do develop below the knee are generally not high risk , and indeed, many may resolve spontaneously with no treatment. Worst of all the diagnostic accuracy of ultrasound falls precipitously as veins get smaller in the lower leg. In 160 medical inpatients who had an ultrasound and a gold standard venogram, the positive predictive value of an ultrasound for a lower leg/calf/distal vein clot was 50%. To reiterate – a positive result on a leg ultrasound has a flip of a coin’s chance of being correct, but it does allow the hospital to document a clot in the leg vein (also known as a Deep Vein thrombus (DVT)) as present on admission, and make any actually clinically meaningful DVT that subsequently develops not count towards the all important hospital acquired numbers. The added benefit of documenting more DVTs in your medical inpatients (as opposed to the post-orthopedic surgical patients) is that it makes patients appear sicker. This matters because another metric- the all important US News World Report rankings – are based on the difference between hospital expected and observed mortality. The higher your expected mortality, the better.
It is not even clear that the numbers, if accurate, would tell the whole story regardless. Consider the feared complication of DVT is a clot that spreads from the leg veins to the heart and causes death – a pulmonary embolism. As far as I can tell, this information is not being publicly reported, but data for the incidence of pulmonary embolism is available from administrative claims data. One would think that the reduction of DVTs should have lead to fewer PEs being diagnosed. Unfortunately, very little in health care is predictable or intuited. The incidence of PE’s has actually dramatically increased since 1998. Our ability to find clots in the lung dramatically improved in 1998 with the introduction of MultiDetector Computed Tomography. This would be ok if finding more PEs results in improved patient outcomes, but it has decidedly not. Mortality from PE is stubbornly unchanged from prior to 1998 to now, ostensibly because we simply got better at diagnosing PEs that were never going to bother the patient.
The point of this long discussion on the blood clot example Binder et al raised is to demonstrate the absolute utter meaninglessness of the metrics highlighted as an example of success. I am relatively certain we can ‘fix’ the overdiagnosis of PE problem by publicly reporting PE data. I am sure the hospital/physician administrator class will respond with some non-granular edict that will strip the physicians ability to order an MDCT for PE. As history would suggest, fewer unneeded CTs will be done, but fewer needed CTs will be done as well. Medicine used to advance organically from the bottom up by education and discussion informed by data. 50% fewer coronary stents are placed in the elective setting over the last decade not because of public reporting or leapfrog, but because the data brought the frequent practice by cardiologists into question.
Binder et. al go on to highlight the benefits of transparency in improving outcomes in New York state patients undergoing cardiac surgery. Apparently, public reporting of outcomes in cardiac surgery patients in New York lead to advances in cardiac care that saved lives. Its a remarkable statement because there is ample data to suggest that lower mortality with public reporting in this setting related to lower surgical volume driven by a fear of operating on sicker patients.
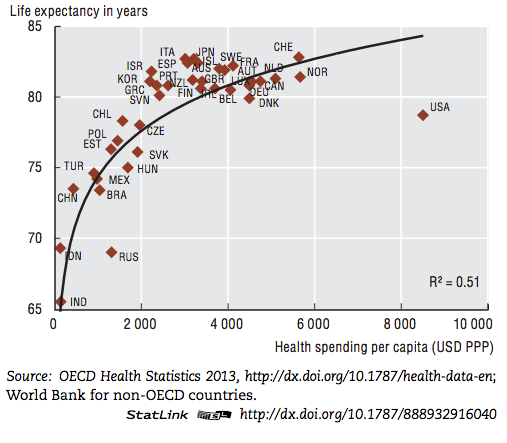
One is left to contemplate the credentials of these arbiters of value in health care. How can we possibly evaluate those who have anointed themselves as gods of value? Data is no longer sufficient to rebut the movement because the data no longer fits the narrative. It should be somewhat discomforting that this chart depicting the United States as outlier when it comes to dollars spent for life expectancy achieved is essentially unchanged since the Leapfrog group came into being in 2000.
The value based movement as currently envisioned has failed. Apparently, a maze of third party payers and third party consultants don’t actually make healthcare better or less expensive.
The authors seem to understand the weakness of their arguments by ending their article with a warning about returning to the fee for service that brought us to the abyss. Fee for service is the culprit that has produced ‘waste, heavy cost, and quality of care issues’, after all. This is all true, but do the authors really believe that the fee-for-service system that existed brought no good with it? It is certainly true that the last half century produced a health care system emerged that was incentivized to treat patients. Great waste arose as a result. But this is the same health care system that finances cardiologists on call to open up your blocked artery within 90 minutes of where you currently sit. It is also the same system that refused to give up on rare, fatal diseases in children when other systems have. It should be lost on no-one that the value based movement has morphed into a tool to strong arm physicians into giving up on those it is cost inefficient to treat. Burned by the managed care experience, third party payers have found a way to make physicians the deniers of care – employ the vast majority of physicians, and tie financial reimbursement to value based outcomes that incentivize doing less regardless of patient need. A generation of physicians now emerges with an allegiance to populations and health systems, so it is no surprise that a good physician today is one who can provide a disney land experience to the consumer, all the while keeping length of stay in hospitals low, while documenting all possible diagnoses in EPIC to maximize patient expected mortality and maximize billing.
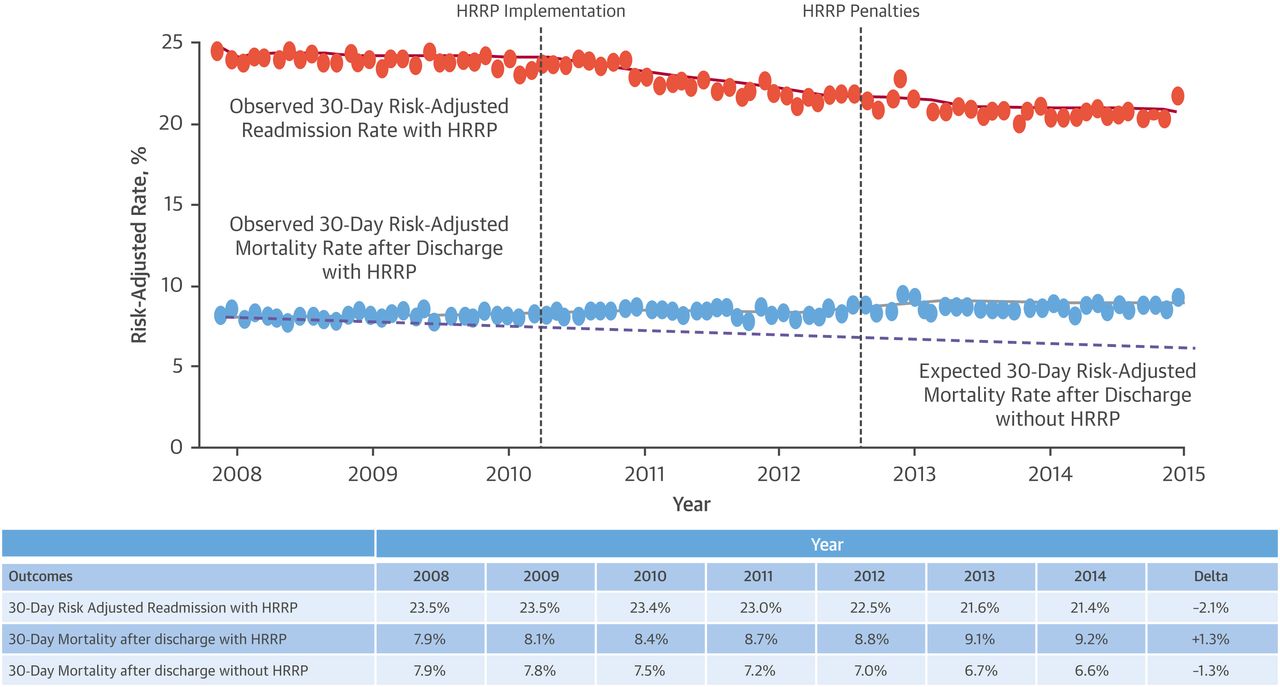
The best thing a customer with a sick heart who made the mistake of being admitted to the hospital with heart failure can do in 2017 is die. Mounting evidence recently lead to leading heart failure physicians to write emphatically that hospital readmission reduction program is associated with fewer readmissions and more deaths.
Waste may abound in our current health care system, but the strategy employed by the value based seers exacts a heavy penalty on our sickest and most vulnerable. Ideologues should consider that we indeed do have a health care system that resulted in too many heart transplants, but is it really better to live in a world where deserving patients don’t get a heart transplant?
This does not mean to say that massive waste does not exist in our health care system. As an example: Hospitals have become massively bloated entities that innovate by hiring patient experience officers, giving patients ipads, paying hundreds of million dollars for EHRs that make physicians less productive, and hiring an army of hospitalists to check boxes and reduce length of stay. I do mean to say that the current plan to give the nations dollars to insurance companies, health care consultants, and non-clinician administrators and expect an intelligent path forward is improbable.
A more honest path appears courtesy of true mavericks like the founders of the Surgical center of Oklahoma that accepts no third party payments but delivers care for elective surgeries at massive discounts relative to regular hospital systems. Any surgical complications are covered free of charge. Patients traveling from a distance have their airfare paid for and are put up in a hotel. Sounds like patient, centric value based care to me. How could this possibly happen without the Leapfrog group being involved?
I realize that the Surgical center of Oklahoma does not have to keep an ER open 24/7, and doesn’t have to pay for interventional cardiologists to be available constantly, but there is ample evidence to suggest the dollars being spent in hospitals are being spent on a variety of goods that have nothing to do with patient health.
Is it a pipe dream to believe that in the wealthiest country on earth we can have a robust private system that can deliver us CAT scans for $400 and still manage to provide a support system for those financially destitute? We currently find ourselves hostage to a health care system that has convinced us that health care is unaffordable, and that keeping the lights on in your local hospital requires being paid $50 for an ECG. The solution has been to create a whole bureaucracy of measurers that have just as much expertise at valuing Big Macs as they do healthcare. The evidence we didn’t need to generate now tells us we don’t measure value well, and it has not resulted in a net reduction in cost or any significant increase in real value delivered.
I would suggest we refocus on the problem at hand. We can start by labeling the current value based movement with the cliched yet appropriate moniker: #FakeNews
Anish Koka is a cardiologist based in Pennsylvania
Categories: Uncategorized








Excellent article. on the high costs and some good ideas on how the cost can be brought down.
“Most Medicare members can barely afford the current system. They won’t be able to afford exposure to additional balance bills”
Funny how you can say that with such certainty in the context of ‘balance billing makes it impossible for most Medicare members to get needed surgical care’.
I practiced at a time when balance billing was the norm and I treated many Medicare patients that were poor. I don’t remember them not having surgery. Why is there such a disparity between what you say with certainty about what would happen and what actually happens?
Your next step was to provide an anecdote about a colleague who had a lot of money and ended up having a balance bill of more than you might like. That was his choice for there are plenty of surgeons today working with Medicare patients that do the entire surgery for a small fraction of what your colleague paid in cash. Your anecdotes are ridiculous because they are relatively well-heeled individuals that have chosen their practitioners based on what they perceive to be the best medical care and they are willing to pay for it.
” would like to hear from Steve2 and Anish on this”
It is your type of thinking that has brought us to the brink of disaster on the healthcare front. I’d like to hear from both of them as well, but if Steve provides hard data then he should be willing to provide the source something he refuses to do in many of his discussions.
My opinion about Medicare balance billing won’t matter. CMS would make that decision with input from Medicare Advantage insurers, doctors, the AARP and probably MedPAC. Most Medicare members can barely afford the current system. They won’t be able to afford exposure to additional balance bills which could be substantial in the case of surgical procedures and cancer treatment.
A former colleague needed a hip replacement a few years back. The surgeon didn’t take our insurance and he charged $17,000 for the procedure. My colleague received $11,000 from our insurance plan for the procedure which was its network rate at the time. He had to pay the other $6K. He could afford to do so but most people can’t. That’s the problem at least for the expensive stuff.
I would like to hear from Steve2 and Anish on this as they are both very smart guys who are in the trenches everyday.
Barry, even though your statement isn’t exactly correct, NYC is a unique area because of the concentration of patients and well-known institutions. Are you advocating physicians leave the system? Are you advocating physicians stop accepting Medicare? Will you permit physicians to accept Medicare for all their present patients and bill all new one’s cash? Are those taking cash the best physicians? I have a lot more questions, but you sidestepped the issue and focused on a particular location instead.
What about the rest of the country? I’ll repeat the statement:
“Barry, on the one hand you wish to have some sort of rating system for physicians. However, you are not willing to pay more for those with the best reputations. There is a disconnect in that type of thinking. “
Are we now talking about getting rid of the relatively few rotten eggs or are we still talking about a rating system?
How do we get rid of bad plumbers?
In NYC, a lot of the most experienced surgeons don’t take any insurance including Medicare. Commercially insured non-Medicare patients can submit their claim, get reimbursed at the contract or out-of-network rate and pay any balance out of pocket. That’s fine for patients who can afford it and are willing to accept it. If the doctor accepts the insurance, though, I think the contract rate should be the full payment at least outside of primary care. If that’s not good enough, don’t accept it and see if you can fill your practice with self-payers.
As for the rating system, if Anish is correct in his statement that most variance in surgeons’ ability is “above the competence bar,” it implies that most surgeons are probably “good enough” assuming the surgeon does enough procedures to keep his skills sharp. A rating system might still be desirable but we could wind up talking about the equivalent of the difference between a four star and five star hotel with a tiny number of “rotten eggs” scattered throughout the system. It would be nice to be able to avoid those.
Balance billing or paying more to a more experienced physician: “ I’m not OK with it for expensive surgical procedures and cancer treatment ”
Barry, on the one hand you wish to have some sort of rating system for physicians. However, you are not willing to pay more for those with the best reputations. There is a disconnect in that type of thinking. One can’t deal with a lot of the other issues you mention until this issue of compensation is cleared up.
Allan, insurers will always pay most of the cost of the expensive procedures like surgeries, cancer treatment and organ transplants. It’s perfectly reasonable that they negotiate reimbursement rates with providers on behalf of their policyholders. I know you think doctors should be able to balance bill and I’m even OK with that for primary care. I’m not OK with it for expensive surgical procedures and cancer treatment and I’m certainly not OK with it for care that must be delivered under emergency conditions. If there is no meeting of the minds on price before services are rendered that’s more than the insurance reimbursement, there is no enforceable contract and patients shouldn’t have to bear the time and expense of going to court to affirm that position.
With respect to physician referrals, numerous magazines publish annual lists of best doctors in their regions. I have no idea how they make those determinations and would like to learn more about how they do it. Maybe that approach could be more widespread. I’ve never heard of doctors suing the magazines because they didn’t make the list.
As for patients being almost completely insulated from the cost of care, I’m fine with high deductible insurance plans, at least for the upper half of the income distribution. A huge percentage of the population can’t afford unforeseen bills of $5-$10K because someone in their family needed to go to the ER for what turned out to be something fairly minor. Lots of people actually have high deductible plans now because that’s all they can afford or that’s the only option their employer offers now.
The good news is that healthcare cost growth is slowing. Medicare spending was only up about 4% in fiscal 2017 or about 1% on a per capita basis. Health insurance companies continue to see medical claims growth come in somewhat below what they priced for which is a big reason why their stocks are doing so well recently. United Health, for example, said on its recent earnings conference call that their hospital inpatient admissions per thousand members declined for the 9th straight year! That’s a positive secular trend in my book.
Barry, you are taking positions on both sides of the coin both here and elsewhere (above) in part because you are looking for a guarantee and there never is one. Your demand is always that someone else is responsible and someone else like the physician should be working harder. Though I like a lot of what you say, I think you are unrealistic.
You like the idea of a lot of government involvement and having physicians paid based upon rates set by third parties with near total elimination of patient responsibility. Ask yourself the question why any physician should put in the extra time to excel if his compensation remains fixed?
If you can’t afford the 50-100 /month, medicaid dollars foro those who can’t would be much better spent in this construct than the current one.
Take of your central planning hat for a minute – don’t worry about where the doctors will come. They will absolutely come if there’s a market – specialists so inclined can do dpc, the army of hospitalists that currently exist could transition… lots of possibilities. No one wants to do primary care right now because it is unrewarding, and burns folks out. DPC would be a game changer – maybe not every high achieving medstudent/resident will try to do opthalmology/orthopedics…
Atlas MD has family rates that are quite affordable. And compared to what the family of 4 would pay for an ACA silver plan – its a deal.
Even ‘simple’ patients need health care maintenance, lipids, colonoscopy, need to be seen for coughs/colds/ – you name it. And if you want to roll the dice without a dpc doc, and just have catastrophic insurance – go for it. The current bells and whistle bronze plan was $400/month for a health 40 year old, and you still have copays and a $6000 deductible! Why are you ok with that??
The pernicious effects of our overly litigious society apparently go well beyond defensive medicine which drives up healthcare costs significantly. It also makes it impossible for objective physician referral services to recommend doctors based on competence and skill as opposed to merely providing a list of local area doctors and it makes it extremely difficult to remove the ‘rotten apples” from the profession because they’re afraid they will be sued for trying. Even honest references from prior employers are hard to come by because they’re afraid of being sued too if they say anything negative about their prior employee. Sad.
DPC is a fine model from the physician’s perspective and is probably a very good deal for the complex patient who can afford the monthly subscription fee. Healthy patients who rarely need to see a doctor are likely to question the value proposition for them.
More significantly, even if everyone in the country could afford the monthly cost to join a DPC practice, where will all the doctors come from if their panel size is one-quarter to one-third the size of a traditional PCP panel?
Finally, what would a typical family of four pay in monthly subscription fees, especially in our more expensive cities and suburbs which, of course, would be on top of their health insurance premium?
Need to be careful of the world you’re creating. If you want doctors making decisions with cost at the forefront of their minds in current set up where the masters are health systems and insurance companies – you will simply end up with less care of the sick and poor since that’s most cost efficient.
Progress of course in medicine has been made in the sickest with the most to lose (as it should).
You folks already know my thoughts on the matter – DPC is capitated, but has the physician directly answering to the pt – docs in that setup are highly incentivized to take very good care of their patients, and still pay attention to a medication that lowers cv mortality .5% over 5 years but costs $1000/month.
” from a patient’s perspective is that the profession has done a poor job in weeding out its “rotten apples” which are, as you say, comparatively rare.”
This would be a very desirable thing for everyone, but how do you believe the profession can weed out its “rotten apples” without running into trouble with the law and without being sued?
“Don’t we have at least some responsibility to help make sure our patients get a good return on the money they spend?”
Yes, especially now that healthcare costs are approaching 18% of GDP. Historically, doctors didn’t perceive it as part of their job to know or care about costs unless the patient specifically brought it up as an issue for him or her.
As for price transparency, the patient needs to benefit directly from a lower price, not just indirectly in the form of supposedly lower insurance premiums than would otherwise prevail. Tiered insurance networks could create a direct patient benefit in the form of a significantly lower copay. Reference pricing could impose a direct penalty for choosing a provider that’s more expensive than the reference price. None of this applies, of course, for care that must be delivered under emergency conditions.
You answered your own question- I’m all for local efforts as you seem to have done with AKI. This is how progress in medicine has been made – organically and bottom up (a relative term). I think progress would be faster with physician lead systems that were competing for patients. Fairly sure the surgery center of OK is incentivized to lower wound infections because they’re paying for the complication.
Though I question this idea of never events. What do u mean by AKI is 0? CLABSI rates are
zero in many units
because of labeling..
Decrease in elective coronary stenting down 50% from 2007 – 2017, not because of some mandate but because of wide dissemination of a paper confirming what many thought.
And steve, I don’t understand your cost comparison. Are you saying that you charge rates for procedures lower than what commercial insurers pay?
“I am finding that once we start measuring stuff, it makes us realize how big a problem we have,” Yes!…that is the way to increase quality/efficiency and reduce costs. Done at the operational level and best if adopted voluntarily. The problem is when bureaucrats (government based mostly) impose measurements and penalties from far above…..almost always turns out to be ham handed with unintended consequences…the tx turns out to be worse than the disease.
When prices have been made transparent, it hasn’t affected spending very much. I know you guys don’t want to believe that, but that is what the health care policy to date has shown. It is what we have seen with our efforts. We list comprehensive pricing for most of our surgical procedures. Most of them are in line with what the OK guys charge, and they are a surgicenter while we are a hospital. It has not resulted in a big change in market share. Price transparency alone doesn’t seem to change much. Living outside the third party payment system? How many people can really afford that? Ever looked up how many people have more than $1000 in a savings account?
“I think if we had measured more in our history, progress would have been much slower…”
I am finding that once we start measuring stuff, it makes us realize how big a problem we have, and pushes us to try to fix things. It lets us see if our fixes are actually working. So, we started looking for AKI, and found we had a higher than average rate. We made up a plan to fix it, and monitored. Not much effect. Made some more changes, monitored, and now we have almost none. Patients doing better. Costs down. Our neighbor hospital took your approach. They didn’t even look for AKI. They didn’t think they had a problem. Then they started looking.
Pharma? Why is 12% OK? What if we still got the same results at 8%? I think we should looking at ROI. Don’t we have at least some responsibility to help make sure our patients get a good return on the money they spend?
At any rate, if you aren’t going to measure stuff, you still haven’t told us how you expect to improve things.
Steve
“Positive outcomes” after surgery can be just as much due to the anesthesiologist, radiologist, pathologist, scrub team, floor nurses, on-call docs, hospitalists – how are you going to choose them?
“physician referral services that can do more than just provide a list of doctors in the area? Why can’t they make some judgments about which doctors are highly regarded by their peers and which aren’t?”
Law-suit city – they’d be gone over night. Which is why physicians are so afraid of disciplining their peers.
Just curious – how do you choose a lawyer? an accountant? a priest?
We need prices to be transparent to those paying for the services. As you know healthcare works in part because the patient is insulated from the prices being charged. I’m not an absolutist, I don’t want folks trying to price shop when they’re in liver failure, or have an elephant sitting on their chest – I would like folks to know what their elective knee replacement costs prior to signing up for it. The innovation, I think for the OK guys, is having one upfront all inclusive bill, and essentially living outside the third party payment system.
I agree with you – re: medical progress. Difficulty is to isolate rent seeking behavior and not throw the baby out.. Pharma is not a very good example of rent seeking – for 12% of total hc cost they return miraculous therapy every 10 years…
I think if we had measured more in our history, progress would have been much slower… https://thehealthcareblog.com/blog/2016/11/18/randomized-trialomania/
Why would you need the hospital’s contracted rates if they are going to charge you a single price for everything, just like the OK guys? At the surgicenters where I work they will tell you the costs if you ask.
Fair question, and since there are no studies on this kind of question can just give you my opinions. First, we benefitted greatly from the arrival of Medicare. Once it was here, we could afford to pay for the care of older patients, and this really opened the floodgates for new diagnostic tools and treatments. If you weren’t going to get paid to do caths or for MRIs, that tech was not going to evolve. Next, we advanced by overpaying for everything. We paid for anything that some provider said worked (forgive the mild hyperbole) even absent real evidence. Then, we largely failed to measure and monitor those outcomes. Fortunately, most people in medicine are ethical and really do mean well, so we advanced, if haltingly. However, it also meant thousands of recalls of devices and the persistence of procedures and therapies that have a poor ROI, or may just not work. And the bad part is that no one cared that much when medicine was 6% of GDP.
Now that medicine is 18% or so of GDP, we need to care. Big business is very much involved in medicine. They are willing to charge hundreds of dollars for generics that cost less than a dollar to make. They push the constant turnover of new devices, w/o much evidence that they are clinically better. (They might reach that p < 0.05 number, but we know that clinically, that is often meaningless.) Pharma is pushing meds that costs hundreds of thousands of dollars, sometimes with little real effect. All of this while we still aren't that good at treating some of our common chronic diseases like diabetes, maybe because we just follow the fad of the day and aren't that good at actually measuring what we do and adjusting when we find what we do isn't working.
So again, if you are advocating that we not measure what we do and then expect people to perform against those measures, what is your alternative? Do you want to just assume everything we do works and every provider is above average?
Second question- So how much further do you think medicine would have advanced if all along we had been better at measuring what we do? Suppose that rather (just to take one example) than take the word of the pharma companies that their new drugs were not addictive we had actually measured it?
Steve
I’m glad to hear that the vast majority of surgeons pass the competence bar which is, believe it or not, consistent with my perception. I think part of the problem from a patient’s perspective is that the profession has done a poor job in weeding out its “rotten apples” which are, as you say, comparatively rare. While their numbers are small, they account for a disproportionate share of malpractice and create distrust and uneasiness among patients. It’s similar to cops that use excessive force being protected by their code of silence culture and their union. Even if their numbers are small, it sows distrust in the community and hurts the reputation of the entire profession.
I agree with you about the importance of a good primary care physician. For years, I didn’t have one locally after my original primary care doctor died. My NYC based cardiologist also does lots of primary care including our corporate physicals while I was still working. Many of my colleagues went to him for that and for general primary care needs and everyone raves about him. The man seems to know just about everything and, as I noted, has an excellent referral network.
As for quality metrics, I think the use of timeouts and checklists in the OR helped to reduce egregious errors like wrong site surgery while definitive protocols to insert a central line helped to reduce CLABSI’s. I also think that to the extent we have quality metrics, there should be much more physician input into their development and feedback that’s taken seriously once they’re implemented. Maybe we could have a deal consisting of less onerous quality metrics and other documentation and administrative requirements which doctors would like to see in exchange for much more aggressive efforts to remove the small number of rotten apples from the profession which patients would like to see.
Find a good primary care physician or find a good cardiologist. You have said many times you have one. How do you know he’s good , by the way?
The vast majority of proceduralists are competent- there is a lot of filtering going on in medical school, residency, fellowship training, etc.
The public should feel safe knowing that surgeons are a fairly select group of folks. The more specialized the surgery, the more exacting the standards. My pointjis that The variance that does exist is mostly above the competence bar. This doesn’t mean there aren’t lebron james surgeons but even if it was somehow possible to genetically engineer everyone to lebron level, lebron isn’t the best player on the floor every day.
I have said repeatedly the physician community does need to do
More about our rotten apples which exist, but are relatively rare. That of course is not the aim of the public reporting movement- and I’m not sure it’s best suited to do that regardless.
There is a lot of local knowledge that used to exist among veteran independent practitioners about who was best suited for a particular need. The era of the vertically integrated hospital means you’re sent to the hospital group with little ability to choose within the group. You learn a lot about someone by golfing with them by the way. Do u golf or spend any significant time with folks u don’t respect?
The best way to promote pwhat’s best for patients is to have a strong independent physician community that answers to patients rather than masters that don’t have the patients best interest at heart.
Ur being hard on the OK guys. Do most surgicenters tell you upfront what the cost of procedures are? And by the way it’s hard to compare ehats actually paid because hospitals won’t disclose their contracted rates.
Let me answer your 2nd question with a question – how did American medicine get this far without quality measures. Do you really think leaps forward in outcomes are going to be as a result of a quality movement that doesn’t understand how to measure quality?
Thanks Steve. That’s very helpful as usual. I’m not looking for the best surgeon meaning one with a national or international reputation for excellence. I’m looking for solid competence, good communication skills and a willingness to explain things and answer my question.
So, my real question is this. If you needed a CABG or a hip or knee replacement and there were 100 surgeons in your region performing these procedures and you knew the outcomes data and the general reputation for all of them, how many of those 100 would you feel comfortable going to for the procedure or sending a friend or family member to? How many of the 100 are middling and should be avoided and how many are so bad that they should be fired or even weeded out of the profession altogether. If the vast majority are solidly competent and do a reasonable number of procedures per month or per year, than patients shouldn’t have as much to worry about as we think.
I needed an ablation in late 2015. The EP that I met at the hospital where I received my diagnosis wanted to treat me for atrial flutter. My cardiologist didn’t consider him that good for what I needed and referred me to a top notch doctor at another hospital system. I was fortunate to have a cardiologist who is really good, cares about his patients and makes it his business to build an excellent referral network including doctors outside of his own hospital’s system. Younger docs would probably feel pressured to keep as much care as possible within their hospital system which could easily be sub-optimal for patients in some cases.
Asking other doctors, house staff, OR nurses and floor nurses will help tell you who to stay away from. It will only sometimes guide you to those with the best outcomes. I get to see all of the outcome data on our surgeons. It is not always obvious. Even then, I am not seeing all of the long term data. We are just starting to get better at that.
In general, I think obsessing over the “best” is not beneficial. Find someone you are comfortable with (if the surgeon with the best technical skills is someone you can’t communicate with, you may not benefit very much from that expertise) who is recommended by people you trust. The surgeon should be willing to tell you how many cases he does and/or the hospital should have that info available. BTW, don’t assume lots of cases is a guarantee of quality.
As an aside, we just took over another failing small hospital. One of the surgeons there is someone we fired, who went to another small hospital we took over (it is doing well now) and we fired him again. He is working at the place we are taking over now, and will be fired again. It amazes me how these guys keep getting referrals.
Steve
“A more honest path appears courtesy of true mavericks like the founders of the Surgical center of Oklahoma that accepts no third party payments but delivers care for elective surgeries at massive discounts relative to regular hospital systems. ”
Again, this is not so true. Hospitals are publishing prices. Their prices are not that much different than the surgicenter. (And they do have to keep cardiologists on call, a tiny part of the costs of having people on call.) Prices at other surgicenters are not that much different. Give these guys credit for great marketing, and for the gullible for falling for the marketing. Mostly, this is just a way for the guys at the OK surgicenter to make a lot of money. (Most of the claims about huge savings are comparing their costs with hospital charges. I hope that at this blog I don’t have to explain why that is a problem.)
Regardless, if you don’t want quality measures, what do you propose? Patients should just assume every doctor is the same? Outcomes don’t matter?
Steve
“My conviction (supported by the large Rand Corporation study of HSA plans) is that we won’t see value improvement in health care unless patients have an opportunity to directly financially benefit from prudent and wise use of health services.”
Paul, you have the key, but those in power don’t want to give much of it to the patient.
“best surgeons are or at least which ones to avoid. I don’t have those contacts.”
I trained at an institution that was well recognized for quality. The Cheif of Medicine had a fabulous reputation yet he thought one of the doctors was one of the best doctors on staff yet the house staff thought he was one of the worst in a hospital filled with great doctors. I had my own choice of who I would use for my family and it was different than who others selected. Then we have the giants who become known as giants as their skills decline. Add to that the problem that different situations are handled better by some than by others.
You sound as if you are looking for a specific quality solution for yourself. The best you can do is get more than one opinion on a serious illness, but if there are two opinions that differ how do you know the third opinion will be any better than either of the first two?
Take note that there are sites on the net that list the number of procedures done and the complications that occur for a few surgical procedures.
Anish, I appreciate your comments. I recognize that defining and measuring quality is a huge problem in healthcare and attempts to do so can create unintended consequences as you describe including creating disincentives to be willing to operate on the riskiest and most complex patients.
From a patient’s perspective, however, for a surgical procedure that can be scheduled in advance, I want to maximize my chances of being referred to a good and skilled surgeon who, in turn, can give me the best chance of a positive outcome. If you or your colleagues need a surgical procedure, your inside knowledge allows you to know or easily find out who the best surgeons are or at least which ones to avoid. I don’t have those contacts. How do I know that my referring doctor isn’t just sending me to his golfing buddy who may or may not be the right guy for what I need?
Why can’t there be physician referral services that can do more than just provide a list of doctors in the area? Why can’t they make some judgments about which doctors are highly regarded by their peers and which aren’t? I would like to know how many doctors and nurses a given surgeon has or has had as patients and how that number compares to peers. I would like to know how many of the relevant procedure a surgeon performs each month or each year and how does that number compare to the number that the specialty society deems sufficient to keep skills sharp.
If a patient posts a negative review about a doctor online, why do so many doctors threaten to sue for defamation even if the review is accurate? Isn’t it just a tactic to intimidate patients and try to stifle negative publicity? What can you offer as an alternative to these quality metrics that will give patients the best chance of a good outcome aside from blind faith that his referring doctor will send him to someone that he would be perfectly comfortable going to himself?
For Dr. Palmer,
According to Don Berwick, M.D., Medicare pays $16 Billion annually to the Medical Schools to support the expense of their post-graduate residencies. That funding is skewed by the size of each Medical School’s medical research budget. The under-graduate medical education is supported by a premium paid to the Medical School based on the healthcare provided by the Medical school faculty to their patients who have Medicare. There are no inducements to allocate these Medicare funds based on the portion of their residency positions that are devoted to Primary Physicians. In fact, there are eight medical schools that do not maintain a Family Medicine residency. Finally, medical research grants (government and philanthropy) pay an additional “mark-up” to the Medical school to administer each grant: now about 18%. The government and philanthropy funding is susceptible to all sorts of economic, social and political trends. As a result, the medical schools support their own lobby in Washington, American Association of Medical Colleges. Their headquarters recently moved into a new building. Parkinson’s Law plays on.
I perceive the following. The political discussion of reducing the Federal government’s contribution to our nation’s health spending occasionally focuses on reducing Medicare reimbursement. This would potentially represent a sudden and substantial change in medical school funding. As a measurement of a Medical School’s economics, the University of Nebraska Medical Center here in Omaha is the city’s largest employer. Finally, in modern times there has been a recession every 8 years. We are now 9 years since the last one.
It’s miles clean that our leaders within the Universities, philanthropy, government at all degrees, expert institutions, and business have failed. a few of the 35 OECD international locations, we’ve got the maximum productive and green agriculture industry. sadly, our healthcare enterprise is the least efficient amongst those countries and, https://www.dissertationking.co.uk/ via some requirements (eg maternal mortality), the least powerful.
I have designed incentive employee compensation systems. It is a given those subjected to it will try and game the system….with unintended consequences. You have to watch that carefully. Unfortunately, our health policy experts (even when they are well intentioned corporate representatives) don’t want to recognize that metrics/transparency can backfire.
My conviction (supported by the large Rand Corporation study of HSA plans) is that we won’t see value improvement in health care unless patients have an opportunity to directly financially benefit from prudent and wise use of health services. Almost all our policy experts discount this and remain committed to top down centralized schemes that haven’t worked and have cost hundreds of billions….and even denial of treatment/high mortality as Koka has described.
We have to be skeptical of our health policy experts. As said by Daniel Kahneman in Thinking Fast and Slow “those with most knowledge are often less reliable. The reason is that the person ….develops an enhanced illusion of her skill and becomes unrealistically overconfident.” page 219
From The Home of https://www.onlinegenericmedicine.com/
Welcome to the world of https://www.onlinegenericmedicine.com/, which provides your choice of quality generic medicine and OTC products from all over the world!
If till date you were picking up your pockets by buying expensive medicines, your pain ends here as you just clicked on the most inexpensive online pharmacy. All the products we sell are all consistent and compatible with the FDA standards and are only made by the reputed manufacturers. All your requirements either they are one-time order or require a 90 day supply for your personal OTC products or generic drugs; you are on the right page! You can choose to save money, time and all the other hassle by getting your requirements from our Online Pharmacy conveniently. Make sure to check out our Terms and Conditions before you shop from https://www.onlinegenericmedicine.com/ as they will sum up any questions you shall have. We are a just a normal and straightforward company looking out for optimum results with minimum prices on your prescription prices that you are looking for. Our motto is to provide all our customers some great experience. We have kept our prices down for you so that you can save the money you deserve.
Good work Dr. Koka! Love the example Surgery Center of OK is setting. May we all be as visionary as they are.
Great article. I thought sc heparin upon admission and daily while in the hospital contributed to the significant drop in DVT and PE or embolic stroke in those with a PFO.
I join the chorus, “well-said!” Historically, the only time in the last 25 years that health spending did NOT increase faster than economic growth was from 1994 through 1999. See health spending reports at http://www.altarum.com The excesses of the HMO era did apparently restrain Parkinson’s Law. When the HMO presence disappeared, there was a huge rebound in our nation’s health spending with annual increases above economic growth from 2001 to 2004. Think about it.
.
I have slowly, but now firmly, come to understand that health spending has increased substantially as a reflection of the social adversities that impact the lives of many people, especially those with essentially no disposable resources. The worsening levels of obesity, young adult suicide/homicide mortality, opiate/gambling addiction, social mobility that is restricted by poverty, and the apparent declining connection of C-Suite governance and social responsibility — are all beyond the control of the front-line health professions. It is clear that our leaders within the Universities, philanthropy, government at all levels, professional institutions, and business have failed. Among the 35 OECD nations, we have the most productive and efficient agriculture industry. Sadly, our healthcare industry is the least efficient among these nations and, by some standards (eg maternal mortality), the least effective.
What can one say other than … Good Job, but how do we extricate ourselves from the monsters we have created?