One thing the health care industry should admire about Wall Street capitalists is their ability to define their target and measure how well they are doing in achieving their aim. Most people would agree the aim of capitalism is profit (saying nothing of whether that is the right aim or not). The measures of that aim are reasonably straightforward using a standardized language of accounting rules. These standardized rules make it easy to compare one business to another using financial ratios (e.g., profit margin, return on capital, return on assets, etc.). When armed with knowledge of the rules and data to compute the financial ratios, deciding what to invest in becomes fairly straightforward—you invest in the opportunities that drive the highest profits over the shortest period of time.
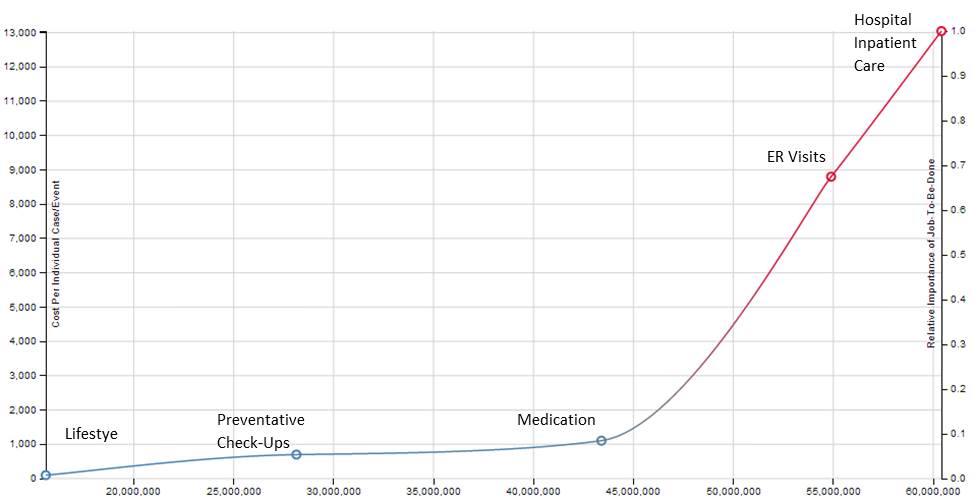
What is the aim of health care? Many of us would say it is health. If that is the case, however, we have been rotten resource allocators. Take diabetes, for example. In 2011 there were over 60 million care events in the US related to diabetes. The cost per episode is plotted on the chart below. It clearly shows (not surprisingly) that the sicker you get, the more expensive your care is. This is not to say that we shouldn’t spend anything on very sick patients. What it does indicate is that though we say we value health, we actually choose to spend our money on sickness.
What would need to change to aim the health care system at health (vs. sickness) and effectively measure our returns on that investment? Here are a few thoughts:
1- Institute a common language for measuring health (and return on health investment)—Countries with developed capital markets almost always have a regulator that imposes a standardized language for financial measurement and reporting. In the United States this regulator is the Securities and Exchange Commission and the standardized language is Generally Accepted Accounting Principles (GAAP). Professor Regina Herzlinger of Harvard Business School has advocated for an ‘SEC’ for healthcare measurement and reporting. We join her chorus in advocating for this as a critical foundational need on which to base improvement going forward.
2- Create business models that make money on health (instead of sickness)— Patients have jobs to be done related to both health and sickness. Unfortunately, in the US providers by and large can only be paid for treating sickness, so the incentive to create businesses truly focused on health has been low. That is changing with the advent of new payment models and technologies such as telehealth, remote monitoring, and predictive analytics. We encourage entrepreneurs to ambitiously pursue business models where providers can make money on health care independent of sick care.
3- Drive care to lower acuity settings—As we can see from the diabetes graph above, spending per care event is much lower when those events occur in lower acuity settings. We hope patient and payor confidence in the quality of care delivered for precision medicine conditions will continue to grow and that more and more volume of care will shift to lower acuity settings.
We are optimistic that the next generation will grow up in a world where they will be able to evaluate and invest in return on health investment in the same way we look at margin or return on capital today. We applaud the innovators and entrepreneurs that are laying the groundwork for that future now.
Ben is Sr. Manager of Strategy and Operations, Health Services at Wal-Mart where he uses his knowledge of disruptive innovation to help make accessible and affordable health care a reality. He works with the Clayton Christensen Institute.
Source: Data compiled from Centers for Disease Control and Prevention/National Center for Health Statistics reports, including “National Diabetes Fact Sheet 2011,” “Self-report of Diabetes and Claims-based Identification of Diabetes Among Medicare Beneficiaries,” “National Ambulatory Medicare Survey,” “Summary Health Statistics for Adults.”
Categories: Uncategorized








“Take diabetes, for example. In 2011 there were over 60 million care events in the US related to diabetes. The cost per episode is plotted on the chart below. It clearly shows (not surprisingly) that the sicker you get, the more expensive your care is.”
That’s what Wall Street “value’s”. The sickness ledger is not the profit ledger, that is the problem.
Good luck getting investors to divest of sickness corporations cause it’s the right thing to do.
“What a unique idea, paying physicians to keep patients well!”
I have another unique idea. Let’s pay physicians for value not volume.
There. Done. The healthcare problem sentenced in a sentence.
I think the writers significantly overstate the ability of investors to compare profitability of companies both across and within industries. While companies are required to adhere to generally accepted accounting principles (GAAP) in their financial reporting, there is often significant latitude in how these numbers are calculated. For example, there is a zone of reasonableness in how reserves for bad debts, warranties, obsolescence, etc. are determined. For revenue that comes in over several years as part of a long term contract, the rate at which revenue is booked can vary from one company to the next. Depreciation schedules can vary as well for financial reporting purposes which is different from tax reporting. In short, accounting for financial reporting falls along a continuum from one (very conservative) to ten (very aggressive). The former understates earnings and returns while the latter overstates them.
In the medical field, I’m all for paying providers to keep patients healthy using a capitated approach and I also like bundled pricing where it makes sense such as for surgical procedures. The downside of capitation for providers, though, is that it requires them to assume some financial risk if the cost of treating patients turns out to be higher than expected. Many are not prepared to assume that risk even in large group practices and hospital systems. Insurers have the expertise to assume significant actuarial risk but many and possibly most providers don’t. Maybe more hospital systems and other large provider groups should also become health insurers.
Disclosure: I spent my 40 year career in the money management business.
There are parts of this post that are interesting and there are parts of this post that are original. However, what is original is not interesting and what is interesting is not original.
What a unique idea, paying physicians to keep patients well! Never heard of that one before 😉
LMAO! Well, Wall Street can teach use how to fleece the government and our patients much more effectively. How to stab someone and kill them before they even know it? Hmmm…?
The way I see it, a dead patient does not help me pay the rent, so I try to keep them all well and alive. That is naked Wall Street.
Years of the drumbeat of prevention have only led to higher health care costs. Unless health is intuitive and not associated with utilization, costs will continue to rise. Once you set up “health” as the new profit incentivized growth industry, you will be wondering how to undo those outrageous costs next.
I agree with Allan. You don’t need a physician for health counselling. We know all the things to do to try to prevent heart disease, hypertension, diabetes, etc. We know to use sunscreen and proper clothing to prevent skin cancer. We know we should use seatbelts to prevent more serious injury from auto accidents. While I believe physicians can promote and reinforce these recommendations, a nurse or health counsellor could do a great job of trying to keep people on track.
Now, that leaves physicians time to treat the seriously ill.
Today aside from vaccination what methodologies requiring the services of a physician can you think of that save money offering preventative care? Are you talking about early diagnosis or something else? Physicians treat disease and like everything else, your car included, the older and sicker the more the costs rise.