By TED EYTAN, MD
Last week’s Health Innovation Week in San Francisco started for me with a day entitled “From Data to Information, to Knowledge to Application: How Health Services Research Can Harness Data to Help Support a More Rapid Learning Cycle,” at @KPGarfield in Oakland, California. I was asked to present an example from clinical practice on “Novel Means of Data Generation.”
Kind of a lot to get my head around as since I am not a health services researcher.
I knew that I would be co presenting with Gilles Frydman ( @gfry ) and as I have always learned, even if you don’t know what to do, take a good history, so I went.
The second in my slide is maybe a small reflection of my anxiety over Twitter, thanks to the audience for letting me express it.
Speaking of social media, I really liked the stated approach for the day, “share whatever you like, just don’t attribute it to people.” For me that sets a great tone, so kudos to the organizers for discussing this proactively rather than waiting for someone to ask. With that in mind, I will attribute things to myself only, since they’re my things to attribute…
What I heard a lot of before Gilles and I approached the podium was the word “data.” Lots of times. Where it comes from, how available it is, how easy/difficult it is to use. This is not a bad thing at all, just recognition of what this group of professionals contributes to our health system.
What I learned (and, sort of know) is a reality that more and more data is not coming from carefully created large datasets, it’s coming from people and health care interactions that didn’t exist 10 years ago, such as patients e-mailing their doctors.
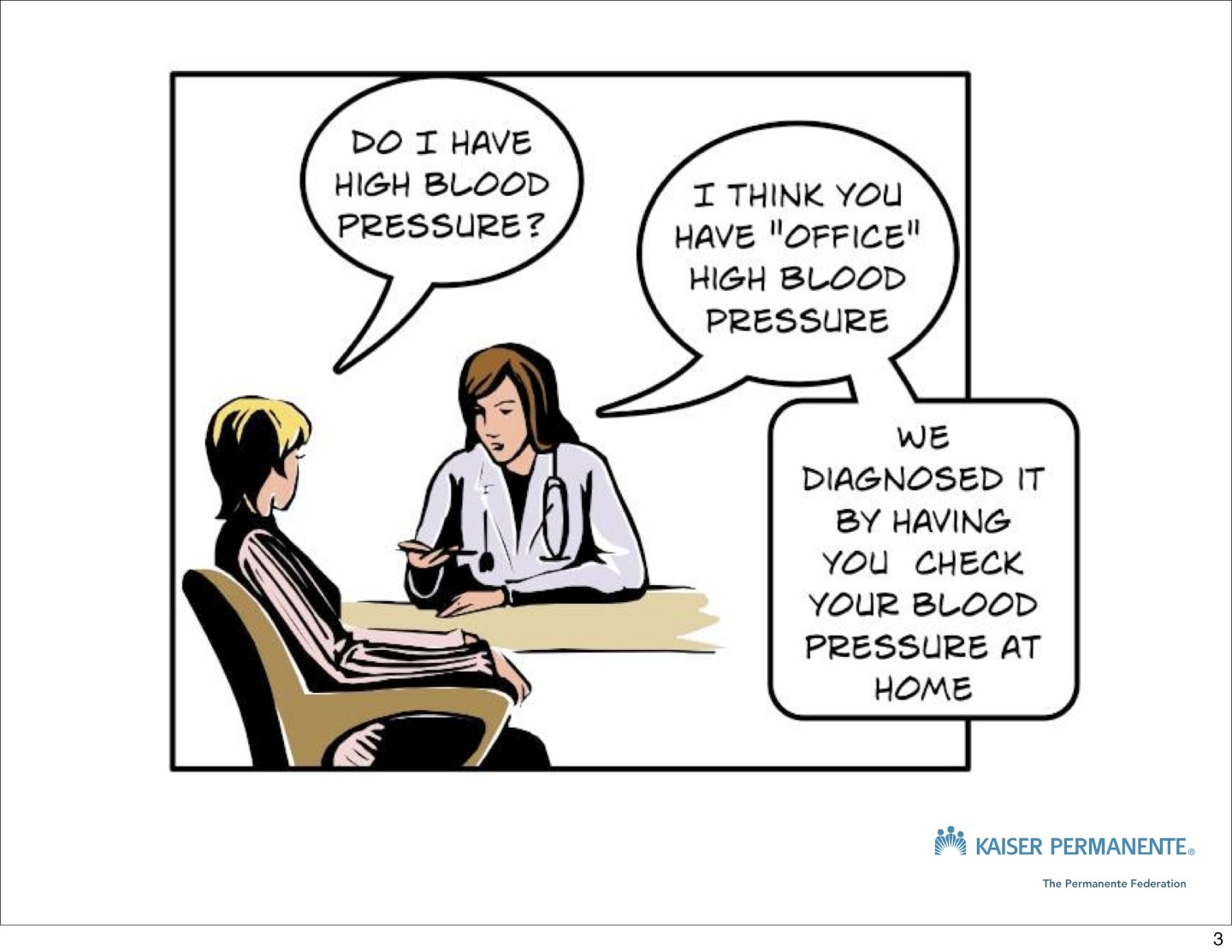
With that in mind, I presented the case study of hypertension, starting with this cartoon that I created previously.:
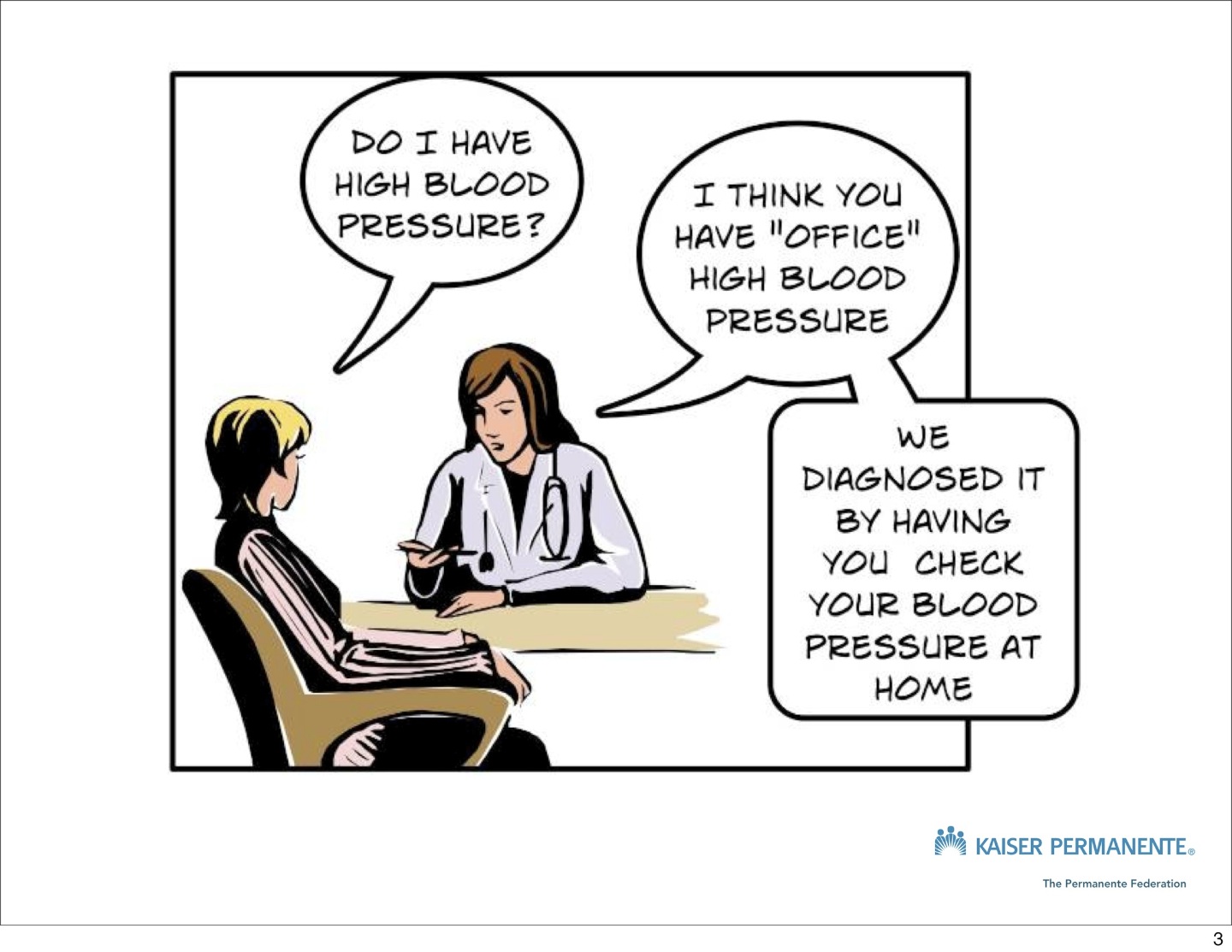
Should this happen more often than it does in health care?
How often does this interaction happen in health care? Not very. Should it happen more often? Probably.
A few issues with hypertension that I illustrated:
- There’s fairly good evidence that blood pressure should not be checked and managed in the medical office, yet it still very much is (#1 reason for visiting the doctor in the United States)
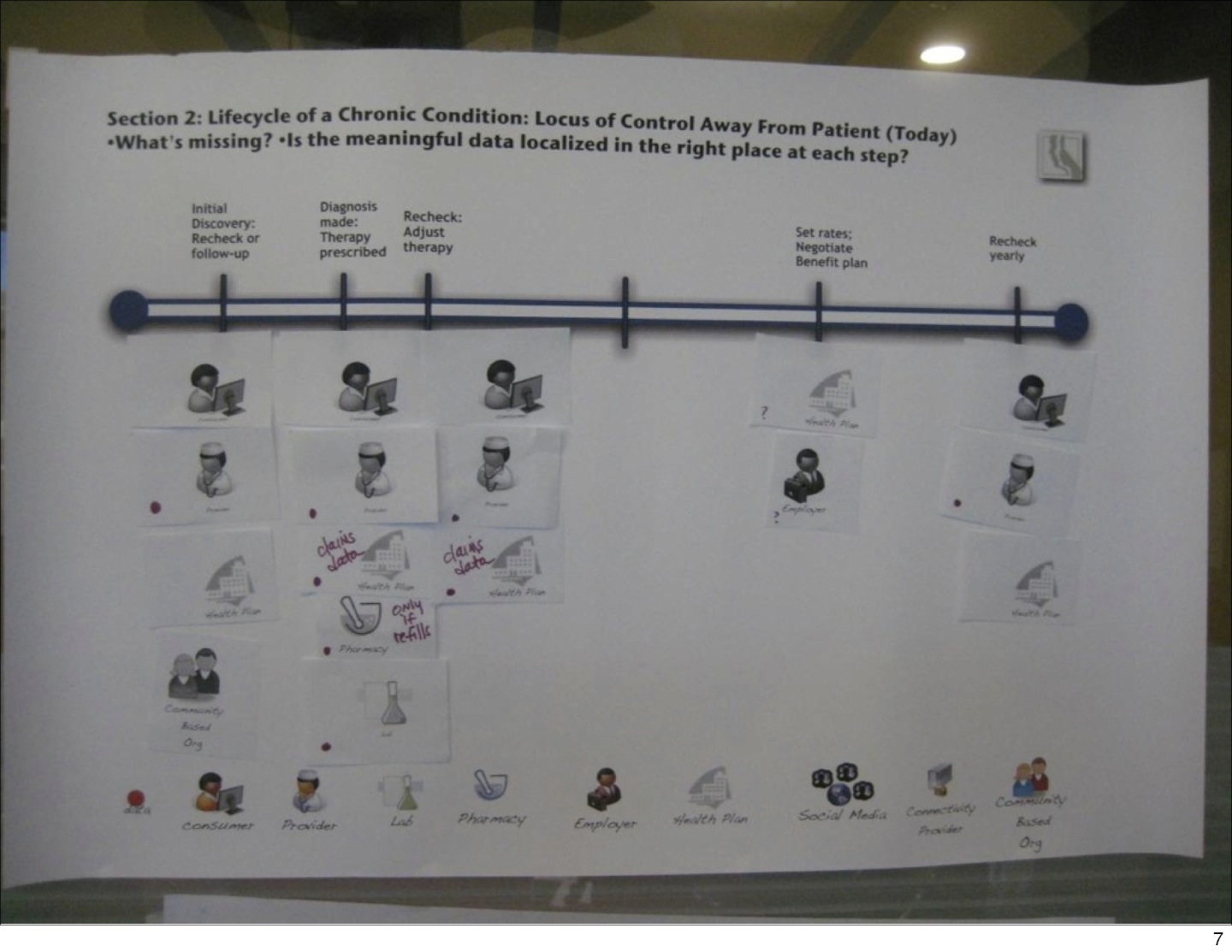
- If you diagram the data flow for hypertension management today, there’s data in pockets/silos everwhere
- The way care is currently organized, it’s sort of linear, with many opportunities for patients to fall through the cracks (and they do, frequently)
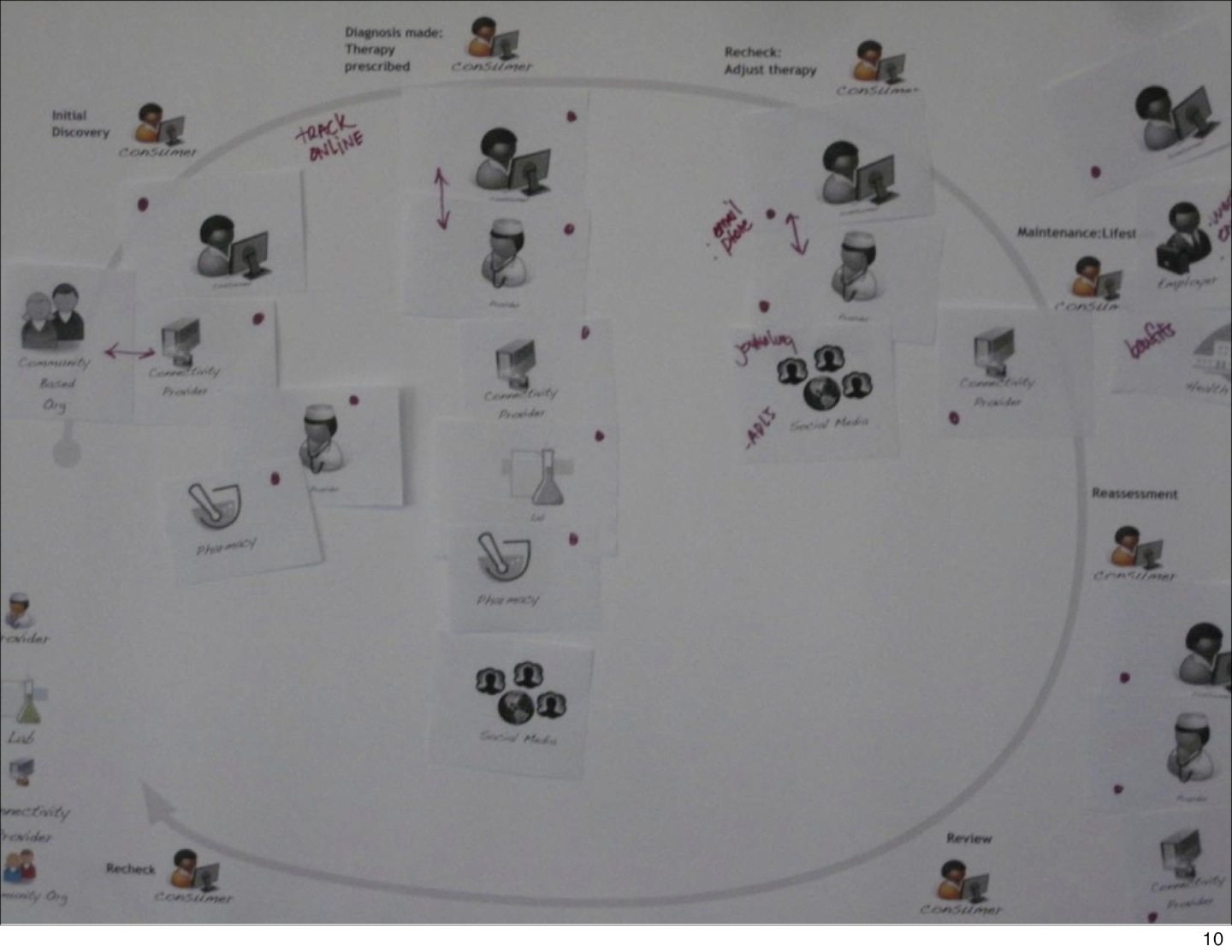
- If patients were to organize the care, they might think of it as a circle/cycle, with them in the center
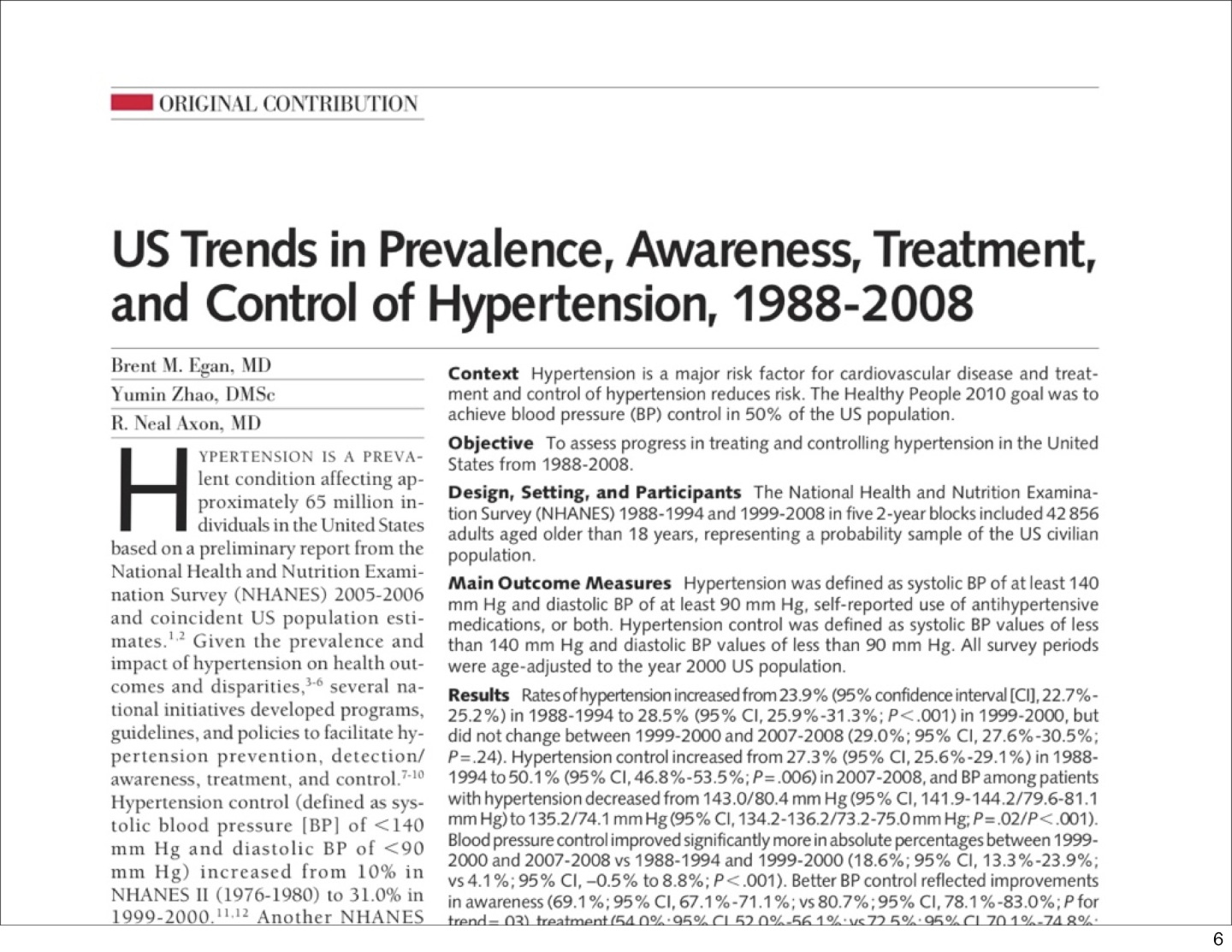
- The best data we have about blood pressure control comes from a very detailed (and very well done) study called NHANES.
- The most recent NHANES data is 2008
- The American Heart Association’s main page for hypertension statistics report data from 2006
- This time frame is something of an eternity in the world of electronic health records / personal health records
- Health Services researchers are looking at these new interactions and drawing useful conclusions – the Group Health Cooperative “eBP” study and recent study by Kaiser Permanente are examples of this.






Our discussion brought me to the biggest question/interest of the day, which was, “How are the people being served by this knowledge involved in the process?” I did not get a good sense that they (patients and families) are, in general. For example, AcademyHealth, the professional society for health services researchers, doesn’t have a patient/family advisory group.
Several innovative data/people applications were presented, including Asthmopolis, the Healthy Community Dashboard for Sonoma County, and Community Data Vital Signs for San Francisco.
The Robert Wood Johnson Foundation’s Project HealthDesign was mentioned and I think it is a good example of a health-services-researcher and patient-friendly approach, because it is looking at new types of data coming from patients, AND involving patients on study teams to help define what’s important in remaking/changing the health system.
Overall, the group and discussion was very stimulating, and very welcoming to non-health services researchers like me, so big thanks for the opportunity to discover an aspect of transforming health care that I hadn’t thought about a lot recently.
Will health services researchers help change chronic illness care (or all care) altogether, by studying these new interactions and the data that comes from them? Will the health services research community follow the trend in the rest of health care to involve patients and families in their work? How will they and who will lead? Are these reasonable questions to ask? Let me/us know in the comments. Also if you were present and want to add your perspective, please do.
Ted Eytan, MD MS MPH, currently works as a Director at Kaiser Permanente, in The Permanente Federation, LLC. His experience is in working with large medical groups and technologists to leverage health information technology to ensure that patients and their families have an active role in their own health care. His clinical interests are preventive care and reducing disparities in health status among vulnerable populations. He is a regular user of social media tools to promote open leadership, and he frequently posts on his blog Ted Eytan, MD.
Categories: Uncategorized








hello TED EYTAN
very nicely explained about hypertension.Points are very informative.
I want more explanation on “Will health services researchers help change chronic illness care ?”
Hello world! I want to share something with you people. I was searching for a consistent <a href=Pilates”>http://greatpilatesnow.com>Pilates exercises | Pilates workout for a few days who can help me doing Pilates workout. But I found no one so good who can provide me with help to build a good physic. I know that everyone needs a good body to execute works with more efficiency. But I hate gymming. So, I took help from this site and now I do possess a good healthy body. Thanks to them.
As more data is collected on patients, there will inevitably be a chance to improve patient treatment by building knowledge that is gained through data mining. The key will be to ensure that there is enough context captured around collected data points so that these factors can be associated with the data. For a blood pressure example, day of week, time of day, and location could all be important factors that would only be known once attributed to a particular patient and a particular measured value.