I’m always on the lookout for advances in healthcare that seem more like 22st century medicine than what we still experience in 2025. Way too much of it seems less advanced than we should be expecting in a world of AI, genetic engineering, nanobots, and the like. I often think of the scene in Star Trek IV where Dr. McCoy finds himself in a 20th century hospital and is appalled:
So I’m pleased to report on a couple of developments that seem like the future.
Transcranial ultrasound stimulation (aka “ultrasound helmet): You may not have ever heard of deep brain stimulation, unless you know someone who has advanced Parkinson’s, dystonia, essential tremors, or epilepsy. It turns out that electrical impulses to certain parts of the brain can help reduce the involuntary motions these conditions can result in.
The drawback is that deep brain stimulation is delivered by electrodes implanted deep in the brain. While this may not be quite as daunting as it sounds, people are still, you know, drilling holes in your head and pushing electrodes into your brain. You can imagine Dr. McCloy’s reaction.
Enter transcranial ultrasound stimulation. A new paper in Naturefrom researchers at University College London (UCL) and Oxford describes using a 256 element helmet to precisely aim ultrasound waves to accomplish the same results.
Our findings reveal this system’s potential to non-invasively modulate deep brain circuits with unprecedented precision and specificity, offering new avenues for studying brain function and developing targeted therapies for neurological and psychiatric disorders, with transformative potential for both research and clinical applications.
Professor Bradley Treeby, senior author of the study from UCL Medical Physics and Biomedical Engineering, said:
Clinically, this new technology could transform treatment of neurological and psychiatric disorders like Parkinson’s disease, depression, and essential tremor, offering unprecedented precision in targeting specific brain circuits that play key roles in these conditions.
The ability to precisely modulate deep brain structures without surgery represents a paradigm shift in neuroscience, offering a safe, reversible, and repeatable method for both understanding brain function and developing targeted therapies.
A little-noticed telehealth safe harbor provision tucked inside the One Big Beautiful Bill was a significant milestone in virtual care. Though it specifically addresses pre-deductible telehealth services in high-deductible health plans, the legislation has far wider implications for both care delivery and insurance design, especially in the commercial insurance market. In fact the permanent extension of a pandemic-era policy is a clear signal to health insurers that a new era of virtual care is under way.
The provision, which permanently extended an expired pandemic-era policy, is a win for employers and workers. After five years of uncertainty, employers are now empowered to provide telehealth services to their entire workforce at little or no cost, which has been shown to reduce access barriers and close gaps in care. For self-funded employers in particular, this flexibility in cost-sharing — combined with an increasingly sophisticated ecosystem of virtual care providers — will further accelerate innovation in benefits strategy and workforce well-being.
Less obviously, this employer-led innovation is also changing the virtual care landscape for a key partner: health plans. Though 20% of employers contract directly with specialized telehealth vendors, 78% rely on their health plan partners — and their vendors — to provide telehealth services for employees. As employers revisit their long-term virtual care strategy with new assurance in the wake of the safe harbor provision, health plans have an important seat at the table.
That seat is heating up, however. In a year when employer healthcare costs are projected to increase by more than 9%, employers are scrutinizing their partnerships and plan design to ensure that virtual care solutions are delivering meaningful value to their employees and their bottom line.
In a new annual survey from the Business Group on Health (BGH), more than three-quarters of employers said they are actively eliminating underutilized programs and underperforming vendors, or are considering doing so. Employers are also stepping up expectations in RFPs, evaluating potential healthcare partners on a growing list of factors and capabilities including performance guarantees, product and network design, reporting and analytics, and member experience.
In this light, the safe harbor provision is a call to action for health plans to evaluate their own virtual care strategy and partnerships through an employer’s lens. Three areas are especially important:
1. Quality
In the BGH survey, employers cited navigation to higher-quality providers and better quality transparency as top priorities — and virtual care is no exception. In last year’s survey, half of all employers expressed concerns about the quality of virtual care.
I have been on a quest to try to understand why I am being charged $34.95 by Labcorp for some lab tests that I think should be free under the ACA preventative care statutes, and for which my insurer Blue Shield of Californian has issued me an EOB with a $0 co-pay.
It’s been a microcosm of the chaos of American health care so far, If you want to catch up here’s part 1, part 2, part 3 and part 4
You may recall that I had paid a $50 co pay for the lab tests connected to my preventative annual wellness visit in 2024 (and I didn’t pay attention) but that when I got a $34.94 charge from Labcorp in 2025 and found that Blue Shield said my copay was $0, I decided to investigate.
I have had a lot of help from Rhea, a senior customer service rep at Labcorp who I think is having nearly as much fun with this as I am. She told me that the co-pay Labcorp tries to collect is the lower of $50 or whatever the total bill is. For the 5 tests I had, Labcorp’s agreed rate with Brown and Toland Physicians (the Blue Shield-owned IPA that contracts with their HMO, of which I am a member) was $34.94. So that is the answer as to that charge.
But it still doesnt answer a couple more questions.
Why was a subsequent lab test I had as a follow up also shown by Blue Shield as a $0 copay on the EOB?
Why weren’t the lab tests I had considered preventative under the ACA and therefore also free?
Rhea’s guess for the first answer is that Labcorp receives a capitated amount for lab tests from Blue Shield or Brown and Toland, and that the second test was somehow covered under that. Maybe, but then why wasn’t the first one?
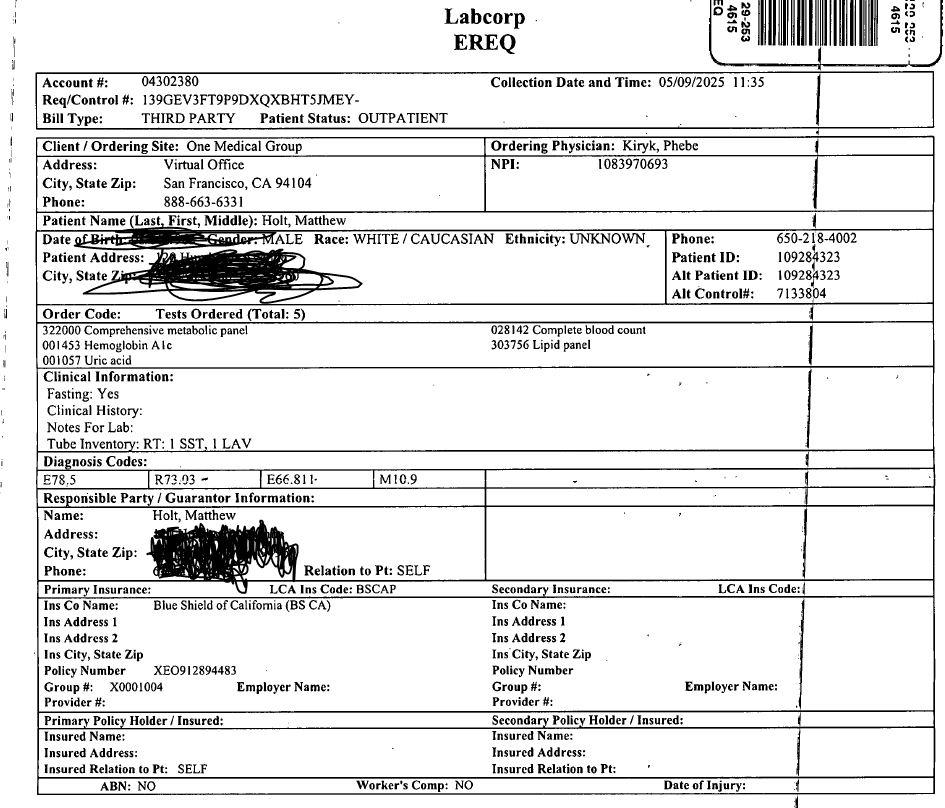
The second question takes me further down a rabbit hole. Rhea dug out the order from One Medical to Labcorp. You can see below that the CPT codes are on it (what the tests actually are) and also what the related diagnosis codes are.
I of course asked chatGPT what those diagnosis codes were and the answer is E78.5 = Hyperlipidemia (i.e. high cholesterol) R73.03 = PreDiabetes E66.811 = Obesity class 1 M10.9 = Gout
As you might suspect as a pretty typical 60+ year old American, I fit the bill for all those diagnoses. The CPT codes for the tests I had are complete blood count, Metabolic Panel, Hemoglobin (A1C), Lipid Panel, and Uric Acid (which causes gout).
Presumably all of those, with the possible exception of the Gout/Uric Acid, could be seen to be preventative. After all the CMS web site explains that preventative screening is free for “Annual Wellness Visits and Physical Exams, for instance with a primary care doctor and Health Screenings for blood pressure, cholesterol, blood sugar for diabetes, and various cancer screenings such as colonoscopies and mammograms”.
So why is this not free to me? Rhea from Labcorp suggests that Blue Shield initially issued me a $0 copay EOB but later should have reprocessed that when it got the bill from Labcorp, and told me to pay the $39.94. She also found that in addition to CMS suggesting what should be called preventative, Blue Shield of CA has a very long document with what it thinks is preventative care. You can see and download it here.
I asked ChatGPT to read it for me and after a bit of looking around we (that’s me and ChatGPT) concluded that E78.5 is in the list of applicable ICD-10 diagnoses codes for Annual health appraisal visits, which are a (free) covered service. So my high cholesterol should be screened for free.
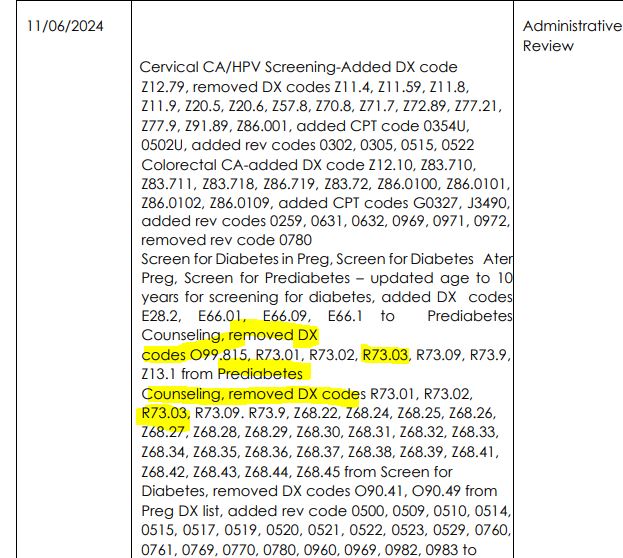
On the other hand there’s a whole section on Page 28 of the document discussing pre-diabetes education but it doesn’t explicitly say that an A1C test is covered under the annual wellness visit. And if you go way down, to page 116, there’s a table that suggests that last year a Blue Shield review removed several of the diabetes codes, including R73.03.
Now I am not going to pretend that I understand what the hell is going on in this document, and why (or whether) Blue Shield is able to change what CMS says it should do–if that is what in fact is happening. But it does seem weird.
And again, because there are no actual costs per test from Labcorp (there are charges per test but they are bundled and discounted on the bill), it’s impossible to tell what the contracted cost for each test was, and therefore whether I got some for free (as I think I should have) and what I was actually charged for.
Finally, I got very excited as Blue Shield sent me a message tonight which had an attachment which I think is a response to the grievance that was somehow filed for me by someone from their executive offices in part 2. But the attachment wasn’t properly formatted. So I don’t know what it says!
No less than I’d expect on this adventure.
But hopefully we are close to finding out who is charging whom for what and why!
UPDATE. I called Blue Shield’s grievance line and a nice customer service rep read me the letter that I couldn’t see online. Essentially Blue Shield has asked Brown and Toland to explain what happened. That grievance will take another 30 days! The rep wasn’t able to send it to me in my portal, but she could send me an email (It will be one of those secured ones that are super annoying to open). She told me it was sent while she was on the phone but 30 mins later, it’s not here!
A Rock Health write-up of this year’s Epic Users Group Meeting captured the artificial intelligence vibe with a play on the names of three new AI chatbots rolled out by the country’s dominant electronic health record firm. “Epic Goes APE (Art, Penny and Emmie),” read the headline, using the first letters of the names of chatbots designed for, respectively, clinicians, revenue cycle managers and patients.
Emmie does positive things for patients – more on that in moment – but at its core the chatbot is a B2B play, designed to address the needs of the hospitals, medical groups and others whose fees have built the privately held EHR firm into an estimated $5 billion business.
Emmie is not an agent of patient autonomy. Its purpose is to help Epic customers (health systems and physician practices) provide more and better services to their customer, the patient, as long as that patient remains a customer.
That context is important. Yes, in a way it’s #PatientsUseAI, but that use is analogous to the AI algorithms deployed by Netflix. While you may marvel at their power of personalization, they’re never going to tell you that the best movie for your particular interest is harbored over at Hulu and, by the way, even if you’re watching tons of programs with medical themes, you’re still a couch potato.
I wasn’t present at the gathering at Epic’s Verona, Wisconsin headquarters, but news accounts and LinkedIn postings suggest that, unsurprisingly for this type of meeting, there was more drama than details. Much of what was unveiled and hinted at – the company said it’s working on more than 200 AI applications – will be rolled out over the course of 2026 and beyond.
Informed by their chart and connected devices, Emmie is designed to support patients between visits. Whether it’s explaining test results in easy-to-understand terms, suggesting next steps, or guiding patients through open-ended conversations about their health, Emmie makes it easier for patients to stay on top of their health and walk into the exam room with a clear picture.
On the clinician side, Art is gathering data from Emmie to get the doctor the information they need before the visit even begins. Art is designed to reduce administrative burden, help doctors better understand their patients, and offer context-informed insights. This can take the form of generating pre-visit summaries, taking real-time notes, and even taking actions like placing orders or verifying prior authorization requirements.
That Rock Health analysis suggested that the real significance “may be less the function and more the channel,” since consumers are far more willing to share health data with their provider – in this case through Epic’s MyChart – than with a tech company (such as an AI vendor). “By capturing patient questions, decisions, and symptom-checking,” Rock Health noted, “Epic gains visibility into information consumers might hesitate to share with a generalist tech company. The EHR giant has already signaled that this data will feed back into [its] tools.”
Or as Epic did not say, “We empower our customers. We empower patients. We empower ourselves.” Good intentions alone do not get your product into use by more than half of all acute-care hospital beds in America, according to a KLAS estimate of market share.
At Healthcare IT Today, veteran tech journalist John Lynn sniffed out the actual schedule for all Emmie’s promised pro-patient wonders. According to Lynn (presumably from Epic itself),
proactive outreach and images is coming in March, 2026
active engagement in November, 2026
future screenings arrive sometime in 2026 (no month given).
Bill payment, scheduling abilities using SMS (texting) and a voice agent are all “coming in the future.”
As I commented on the Epic LinkedIn post, “How about patient-reported outcome measures [e.g. Proteus Consortium’s], whether from an app linked to Epic (i.e., like Twistle by Health Catalyst or others) or the patient’s own wearables?” I tagged Seth Hain, Epic’s senior vice president of research and development, who played a prominent role at the meeting, but got no reply. (To be fair, maybe he took some vacation time after an intense few weeks.)
In a recent STAT First Opinion that took up the topic of autonomy, I asserted that true informed consent means physicians should be obligated to inform patients what Epic’s Cosmos system says about the likely outcomes of treatment for individuals with their clinical profile. Those predictions come from a database drawing on a mind-boggling 15.7 billion patient encounters. But patients should be able to access that information about different hospitals’ results on their own.
At the Users Group Meeting, Epic announced a further refinement of Cosmos, with founder and chief executive officer Judy Faulkner proudly announcing that the company will be able to “predict the future” for patients. (For a deep dive into Cosmos, I recommend the posts of veteran medical informatics expert Mark Braustein.)
Faulkner did what any smart businessperson would do. She spoke about how her company’s product would enable an important segment of customers, clinicians and health systems, to provide better care. What those customers actually do (or don’t do) for their “customer,” the patient, with the Epic software? Evidently “Not my job.”
Michael L. Millenson is president of Health Quality Advisors & a regular THCB Contributor. This first appeared in the “Patients use AI” Substack
Dr Kaelee Brockway is a professor of education and physical therapy who has built a series of AI based “patients” for her PT students to train on. Kaelee is a pioneer in using these tools for training. She showed me the personas that she has built with LLMs that are now being used by her students to figure out how to train their soft skills–a huge part of any training. This a great demo and discussion about how clinical professionals are going to use LLMs in their training and their work–Matthew Holt
“So far AI in health care is being used to drive existing profits on workflows and increase revenue per event that patients in the end have to pay for. That’s not a win for anyone long term!” Included Health’s CEO Owen Tripp dives into the present and future use of AI, LLMs, patient self-triage and self treatment and all that. Another interesting conversation on where patient facing AI will end up — Matthew Holt
You’ll recall we left it with a mystery $34.94 bill which didn’t either fit the official $50 copay amount I have, nor the $0 patient responsibility in my EOB. I got a call from Rhea Fleming, an experienced customer rep at Labcorp, on whose virtual desk this has been dumped. We had a lovely conversation in which we agreed that the co-pay should either have been $50 or $0 but that it’s possible that the co-pay is the lower of $50 or the amount Labcorp was trying to collect.
She had previously called the Blue Shield of California provider line to try to figure this out. Blue Shield had indeed kicked this claim from Labcorp to Brown and Toland the IPA I am assigned to in the HMO product I bought. The charges from Labcorp were $322.28 and the response from B&T was that the contractual price (i.e. what they agreed to pay Labcorp for those tests) was $34.94, hence the “adjustment” of $287.34. However in Labcorp’s system the algorithm interpreted B&T’s response as saying 1) the agreed payment is the $34.94 according to the contract and 2) they were not going to pay so the patient owes the difference. When Rhea Fleming asked Blue Shield’s rep why the patient owed payment on this, the Blue Shield rep said that the procedure code and diagnosis code from my PCP (One Medical) did not count as preventative care. In other words Labcorp has not got paid at all for running these tests so far, because they are according to B&T “not preventative”. Although IMHO, CMS says that they are. And of course as it says my copay is $0 I’m interpreting Blue Shield of California’s EOB as saying that to me!
Hence Labcorp generated the bill for the $34.94 and sent it to me. Which started this whole telenovela.
BTW Rhea’s conclusion was that as none of the tests were “preventative,” Labcorp billed me the $34.94 as that was the total it was contractually owed rather than the $50 copay I am supposed to pay for lab work. I actually checked back in my Labcorp account and found that last year I did in fact pay $50 so perhaps last year I had different tests or somehow they have changed the algorithm. I checked the EOB for that 2024 bill and the total charge was $445.20 of which Blue Shield paid $28.07. No I couldn’t find the Labcorp bill on their system, presumably because I have paid it! Given that I paid $50 for services from Labcorp on that date (yes, it took me 7 months to pay up!), it’s likely that the agreed payment was $78.07 ($50+$28.07) of which I unthinkingly paid the $50 copay. And yes that should have been preventative too. (Perhaps I should ask for that $50 back!!)
BRIEF UPDATE: Rhea from Labcorp looked into this 2024 bill and that is exactly what happened
Then, I had another thought.
It turns out that the lab results this year generated a further concern in my doctor’s mind. (Bear in mind I had the lab tests before the office visit so that we could discuss the results). It seems that my iron levels were a little low, so while I was in the doctor’s office he ordered some more tests specifically about that. As One Medical has techs on site they drew my blood then and there and shipped it to Labcorp.
According to my EOB, Labcorp’s charge for those new tests was $60.79 of which Blue Shield or rather Brown and Toland again paid $0 and created an EOB which again said my patient responsibility was $0. I asked Rhea to check that bill in her system and it turns out that I do NOT owe Labcorp anything on that set of tests. Maybe they were coded as preventative? I tried to find the bill on my patient portal at Labcorp but because I don’t owe anything I haven’t been sent an invoice and without an invoice number you cannot check the bill!
When Rhea ended the call with me, her next move was going to enquire of Blue Shield and Brown and Toland what the reason was for me owing $0 on that bill!
Meanwhile I await the result of the official Blue Shield investigation with interest. Of course this might just have come down to Amazon One Medical coding the tests incorrectly. But it’s all fun and games if you have unlimited patience in American health care.
There is no doubt Robert F. Kennedy, Jr. is sincere about wanting to make the world a better place. The Hudson River cleanup, which he helped lead, is one of the most successful environmental achievements in the United States. It had bipartisan support, set global standards, and earned the highest compliment: imitation.
It was quite reasonable to believe Mr. Kennedy could use those same skills and passion to lead Health and Human Services (HHS). He has a proven track record with complex systems, scientific evidence, and protecting public welfare. Even skeptics of his appointment want him to succeed.
But skill sets in one domain do not always translate to another domain—no matter how strong that skillset is. And it can be very difficult to realize this until the effects of the Law of
Unintended Consequences start to complicate things—as is now happening with Mr. Kennedy’s approach to public health. I know the feeling — because I had made the very same mistake.
Lessons from Databases
I had over fifteen years of experience with databases in auto parts, newspapers, manufacturing, and insurance before I started working with healthcare databases. Each domain had its own complex logic but I could adapt from one domain to another relatively easily.
When I started at the University of Iowa’s Department of Anesthesia, I was confident I could make a smooth transition to a new domain as I always had.
My first assignment was simple: create a report of the active prescription medications listed for a patient at a given appointment. It didn’t take very long to figure out how to find patient data, appointment data, and prescription data. My expertise in databases was transferring to a new domain quite smoothly!
All I had to do was use a chart I had and see how to make the connections.
I can read…how hard could that be?
Not only was it harder than I expected it to be, but I also didn’t immediately recognize why.
Parallel Paths
Mr. Kennedy took a similar path with vaccines and autism. He could see patient data. He could see vaccine data. He could see autism data. The connections seemed clear.
In my case, a researcher at Iowa had a theory that the length of a clinical appointment could be predicted by the number of prescriptions a patient was taking. My job was to combine all of the relevant data. He would then use that for his calculations.
I built a dataset. Everything looked right. But I was so new I didn’t realize there were hidden flags that identified appointment types. And flags for prescriptions that were active on the date of the visit. I didn’t even know there was a database flag that identified them. Flag is an oversimplification; it was far more complex than that.
Kennedy thought he had confirmation of his theory in 1998, when Andrew Wakefield and colleagues published a study in The Lancet suggesting a link between the MMR vaccine and autism. It looked right. It seemed obvious. A lot of people believed it. But like my report, it was flawed — a small sample size, uncontrolled design, and speculative conclusions. My initial dataset had “false” data because I missed some flags. My mistake was caught long before the data ever got close to any kind of study. Not only did the Wakefield study include falsified data, it made it to the publication stage.
My researcher kindly showed me my errors and I was fortunate it was early on in the process. Meanwhile, epidemiologists and clinicians have repeatedly shown Mr. Kennedy where his conclusions don’t stand up. Yet, like a friend of mine who once argued astronomy with Dr. James Van Allen — yes, the Van Allen Belts Van Allen — some convictions are hard to let go of, no matter how authoritative the counterevidence.
Three Questions for Transferring Expertise
I have learned to ask myself three questions whenever I enter a new domain — and I think they apply to all of us…including Mr. Kennedy.
So some of the more outspoken employees have written a letter. That should do the trick.
The letter, which they call the FEMA Katrina Declaration, was signed by almost two hundred current and past employees (although only three dozen allowed their names to be public). They charge:
Since January 2025, FEMA has been under the leadership of individuals lacking legal qualifications, Senate approval, and the demonstrated background required of a FEMA Administrator. Decisions made by FEMA’s Senior Official Performing the Duties of the Administrator (SOPDA) David Richardson, Former SOPDA Cameron Hamilton, and Secretary of Homeland Security Kristi Noem erode the capacity of FEMA and our State, Local, Tribal, and Territorial (SLTT) partners, hinder the swift execution of our mission, and dismiss experienced staff whose institutional knowledge and relationships are vital to ensure effective emergency management.
The letter goes on to list “Six Statements of Opposition,” calling to reverse various actions the Administration has taken that they believe impairs FEMA’s ability to fulfill its mission. Each seems perfectly reasonable, and none seems likely to result in action, at least unless/until disasters strike enough red states to force action.
FEMA spokesperson Daniel Llargues was not impressed, responding: “It is not surprising that some of the same bureaucrats who presided over decades of inefficiency are now objecting to reform. Change is always hard. It is especially for those invested in the status quo. But our obligation is to survivors, not to protecting broken systems.”
I probably wouldn’t have paid much attention to the letter, except it comes two months after some 90 NIH scientists issued their “Bethesda Declaration” to protest what has been happening to the NIH so far in the Trump Administration. Addressed to Director Jay Bhattacharya, it declared:
For staff across the National Institutes of Health (NIH), we dissent to Administration policies that undermine the NIH mission, waste public resources, and harm the health of Americans and people across the globe. Keeping NIH at the forefront of biomedical research requires our stalwart commitment to continuous improvement. But the life-and-death nature of our work demands that changes be thoughtful and vetted. We are compelled to speak up when our leadership prioritizes political momentum over human safety and faithful stewardship of public resources.
The Declaration lists five categories of cuts the Administration has taken, about which they warn: “Combined, these actions have resulted in an unprecedented reduction in NIH spending that does not reflect efficiency but rather a dramatic reduction in life-saving research.”
Amen to that.
Director Bhattacharya was somewhat more respectful than Mr. Llargues in his response, claiming: “The Bethesda Declaration has some fundamental misconceptions about the policy directions the NIH has taken in recent months, including the continuing support of the NIH for international collaboration. Nevertheless, respectful dissent in science is productive. We all want the NIH to succeed.”
I don’t believe him. This Administration does not recognize any dissent as “respectful.”
This is Part 2 of Jason and Gigasheets’ investigation into the Capital Women’s Care vs UnitedHealthcare contract dispute in which (partially at my request) he expanded the investigation to look at other providers in the same market. Revealing stuff!–Matthew Holt
While Capital Women’s Care (CWC) battles UnitedHealthcare over contract terms, a deeper look at Maryland’s OBGYN market reveals a complex competitive landscape where negotiated rates vary dramatically across providers and procedures. By analyzing price transparency data from both UnitedHealthcare and CareFirst BlueCross BlueShield, we can see exactly what each insurer pays CWC’s competitors. The results are eye-opening.
The Players in Maryland’s OBGYN Market
Our analysis focuses on four OBGYN providers in Maryland that have contracts with both UnitedHealthcare and CareFirst. These four practices were selected as a representation of the broader market because they have published rate data with both insurers, allowing for direct comparisons. However, Maryland’s OBGYN landscape includes dozens of additional providers, from solo practitioners to hospital-based practices, each with their own negotiated rates that may follow different patterns.
The four providers in our analysis include:
Capital Women’s Care – The large practice at the center of the UHC dispute, with multiple locations across the region
St Paul Place Specialists (Mercy Medical Center) – Baltimore-based OBGYN practice with established market presence
Maryland Physicians Edge – Women’s health group with OBGYN services, now part of Advantia
Simmonds, Martin & Helmbrecht – Established OBGYN practice, also under the Advantia umbrella
The four-provider sample provides valuable insights into competitive dynamics among major market players and helps contextualize the CWC-UHC dispute within broader industry patterns.
Following our analysis in Part 1, we examined negotiated rates for three common gynecologic procedures:
Code 56515: Destruction of cervical lesion (treatment following abnormal Pap smears)
Code 57288: Sling operation for stress incontinence (surgical procedure)
Code 58558: Hysteroscopy with sampling (diagnostic procedure for abnormal bleeding)
The Rate Comparison: UHC vs CareFirst
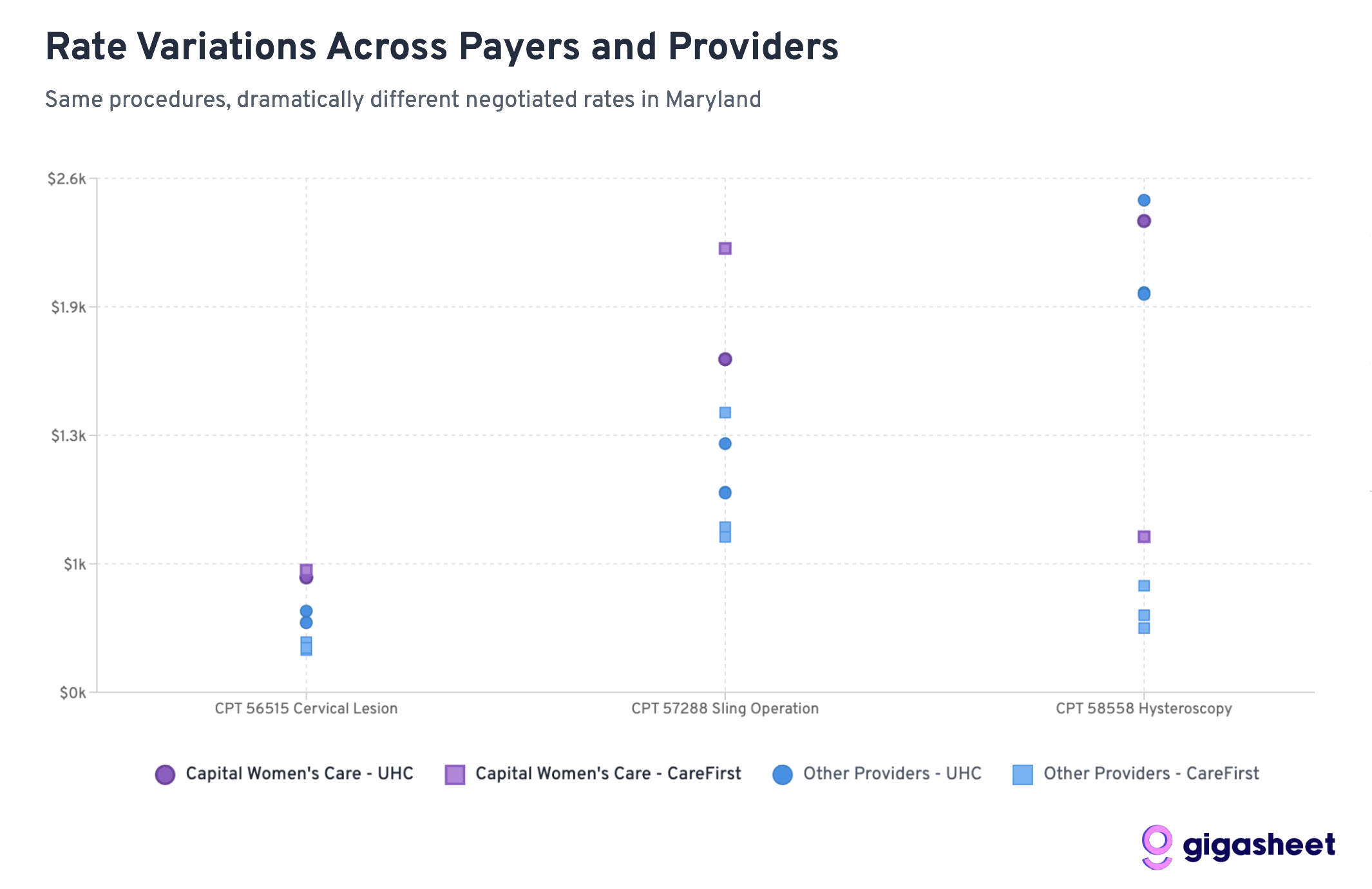
Rate variations in the price transparency data reveals a complex competitive landscape where UHC pays 200-500% more than CareFirst for hysteroscopy procedures across all providers in our sample, while Capital Women’s Care shows mixed positioning. Sometimes Capital Women’s Care commands premium rates from UHC (codes 56515, 57288), other times they’re receiving comparable rates to smaller competitors (code 58558). The data suggests both sides in the CWC-UHC dispute have legitimate arguments: CWC already receives competitive or premium compensation, while rate inconsistencies across procedures indicate room for negotiation.
Extreme rate variations (up to 519%) between UHC and CareFirst reveal market complexity, with Capital Women’s Care showing mixed competitive positioning that supports both sides’ arguments in their contract dispute.
Key Findings: A Tale of Two Insurance Strategies
UHC Generally Pays More Than CareFirst
Across 12 provider-procedure combinations, UnitedHealthcare pays higher rates than CareFirst 75% of the time. This suggests CareFirst has been more aggressive in negotiating lower rates across the Maryland market.
Hysteroscopy Shows the Most Dramatic Differences
For Code 58558 (hysteroscopy with sampling), the rate differences are staggering:
UHC pays 203-519% more than CareFirst across all providers
Average UHC rate: ~$2,200 vs CareFirst rate: ~$510
This represents the largest systematic difference across procedures
Capital Women’s Care Commands Premium Rates
CWC’s rates relative to competitors reveal why UHC may be resistant to further increases:
Code 58558: CWC’s UHC rate ($2,384) is already comparable to competitors, despite CWC’s larger scale
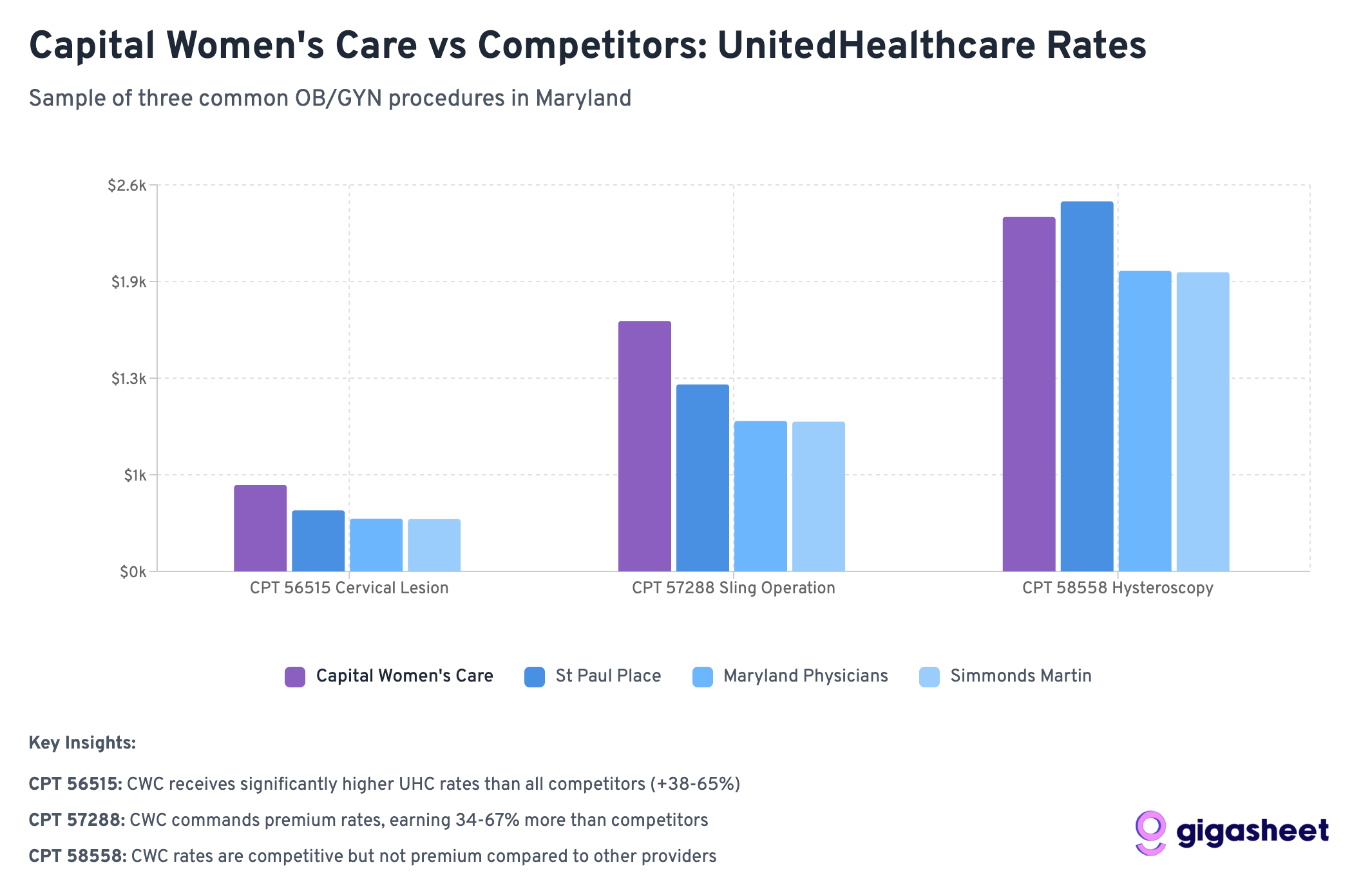
Code 56515: CWC gets slightly better terms from UHC ($581) vs competitors ($352-411)
Code 57288: CWC receives significantly higher rates from UHC ($1,685) vs most competitors ($1,008-1,258)
Wide Rate Variations
The most extreme example: Simmonds Martin & Helmbrecht receives 519% more from UHC than CareFirst for hysteroscopy procedures (a difference of nearly $1,700 per procedure). These patterns suggest that while some procedures have established market rates, others (particularly diagnostic procedures like hysteroscopy) lack standardized pricing, contributing to the complexity of provider-insurer negotiations like the CWC-UHC dispute.
Rate variations reveal dramatic pricing inconsistencies across Maryland’s OBGYN market, with hysteroscopy procedures showing the most extreme disparities difference between the highest and lowest negotiated rates for identical services.
What This Means for the CWC-UHC Dispute
CWC Already Commands Premium Rates
The data reveals a key insight: Capital Women’s Care isn’t necessarily getting unfair treatment from UHC. In fact, CWC often receives higher rates than competitors from both insurers:
For hysteroscopy (58558), CWC gets comparable UHC rates despite being a larger practice that should theoretically have less negotiating leverage
For cervical procedures (56515), CWC receives 40-65% higher rates from UHC than smaller competitors
For sling operations (57288), CWC’s UHC rate ($1,685) significantly exceeds most competitors
This pattern suggests UHC’s resistance to further rate increases may be economically rational rather than punitive.
Industry-Wide Rate Fragmentation
The massive variations between UHC and CareFirst rates across all providers highlight fundamental pricing inefficiencies in healthcare. However, within each insurer’s network, CWC consistently commands premium rates, suggesting their market position is already strong.
Scale vs. Negotiating Power
Conventional wisdom suggests larger practices should receive lower per-unit rates due to volume efficiencies. The data shows the opposite: CWC often receives higher rates than smaller competitors, indicating they’ve successfully leveraged their size for premium pricing rather than volume discounts.
The Broader Market Dynamics
CareFirst’s Market Power
CareFirst BlueCross BlueShield appears to have leveraged its position as Maryland’s dominant insurer to negotiate significantly lower rates across the board. With roughly 50% market share in Maryland, CareFirst can drive harder bargains with providers who can’t afford to lose access to half their potential patient base.
UHC’s Perspective Becomes Clearer
UnitedHealthcare’s position in the dispute gains context when viewed against competitor rates. UHC is already paying CWC premium rates compared to other Maryland OBGYN providers. From UHC’s perspective, further rate increases would create an even larger gap between what they pay CWC versus smaller practices.
The Economics of Provider Consolidation
The data illustrates a key tension in healthcare consolidation: large practices argue their size justifies higher rates due to quality and convenience, while insurers worry about paying premium prices for what should be commodity services. CWC appears to have successfully established premium pricing, making UHC’s resistance to further increases economically understandable.
Looking Forward: What This Means for Healthcare Costs
The Price Transparency Revolution
This analysis is only possible because of federal price transparency requirements that took effect in 2021. For the first time, we can see exactly what insurance companies pay different providers for the same services, revealing the massive hidden variations in our healthcare system.
Market Efficiency Questions
The data raises fundamental questions about market efficiency:
Why does the same procedure vary by 500% between insurers at the same provider?
Are patients getting better care when insurers pay more, or are some insurers simply paying inflated rates?
How can patients make informed decisions when rate variations are this extreme?
Regulatory Implications
These findings may attract regulatory attention, particularly around:
Whether rate variations this extreme serve any legitimate purpose
How to ensure patients aren’t penalized for insurance-provider rate disputes
Whether price transparency alone is sufficient to drive market efficiency
Conclusions: Both Sides Have Valid Arguments
The Capital Women’s Care vs UnitedHealthcare contract dispute becomes more nuanced when viewed through competitive rate data. Our analysis reveals that both sides can point to legitimate evidence supporting their positions:
Capital Women’s Care’s Case:
Rate Inconsistencies: For some procedures like hysteroscopy (58558), CWC receives similar UHC rates to much smaller competitors, despite CWC’s larger scale and presumably higher overhead costs.
CareFirst Comparison: CWC’s significantly higher rates from CareFirst for certain procedures (like sling operations at $2,245 vs UHC’s $1,685) suggest room exists for UHC rate increases.
Market Position Justification: As Maryland’s largest OBGYN practice, CWC can argue their scale, convenience, and comprehensive services warrant premium compensation.
UnitedHealthcare’s Case:
Already Premium Rates: Across multiple procedures, CWC receives higher rates from UHC than smaller competitors (40-65% higher for cervical procedures), indicating UHC already recognizes CWC’s value.
Economic Reasonableness: Further rate increases would create an even larger premium gap between CWC and other providers, potentially making UHC’s network economics unsustainable.
Mixed Performance: The inconsistent pattern across procedures suggests CWC’s premium positioning isn’t uniformly justified across all services.
The Complexity of Healthcare Negotiations:
Rather than a clear case of unfair treatment, the data reveals the inherent complexity of healthcare rate negotiations. Both parties can legitimately point to specific procedures and comparisons that support their position, while the overall picture remains genuinely mixed.
This analysis suggests the dispute reflects broader challenges in healthcare pricing: How do you fairly compensate scale and market position while maintaining reasonable cost structures? The competitive data shows there’s no obvious “right” answer; just different ways to interpret the same complex market dynamics.
The real insight isn’t that one side is clearly right, but that healthcare rate negotiations involve legitimate competing interests where reasonable people can look at the same data and reach different conclusions about fair compensation.
Jason Hines is CEO of Gigasheet which delivers AI-powered price transparency market intelligence.. This was first posted on their corporate blog
Note: This analysis is based on a sample of price transparency data filed by UnitedHealthcare and CareFirst BlueCross BlueShield, as mandated by federal regulations. The rate calculations are aggregations of data from multiple contracts and locations within each provider organization. To expand our rate analysis from Part 1, we resolved EINs to organization names using public data sources.