On Episode 158 of Health in 2 Point 00, Jess and I talk about Datavant raising $40 million in a Series B for their open health data exchange platform, Mira raising $2.7 million for it’s Costco-esque health insurance alternative, Avail raising $100 million providing telehealth for the OR, ScriptDrop raising $15 million for prescription drug delivery, and Abridge raising $15 million to help patients transcribe doctor’s appointments. —Matthew Holt
Above the Fold
Health Professionals Are Tomorrow’s Health Journalists. Here is a Code of Ethics to Guide Us and Trump’s White House Doctor.
By MIKE MAGEE

The patient/health-professional relationship is fundamentally grounded in science and trust, and involves the exchange of compassion, understanding and partnership. The Covid-19 pandemic has challenged this relationship by acutely increasing the nation’s burden of disease, creating new barriers to face-to-face contact, and injecting high levels of fear and misinformation.
Dr. Sean Conley, Trump’s White House physician, in his dodgy and evasive management of legitimate questions from the White House press corps regarding the President’s health, has made matters worse.
As this week’s report on an analysis of 38 million articles on the pandemic revealed, much of the misinformation our citizens have experienced can be traced to a single individual who lacks any health credentials – our own President Trump. Sarah Evanega, the director of the Cornell Alliance for Science and lead author of the report stated, “The biggest surprise was that the president of the United States was the single largest driver of misinformation around Covid. That’s concerning in that there are real-world dire health implications.”
The solution to that specific problem is only one month away – vote him out. But if Trump can be successfully sent packing, how prepared are our health professionals, in the face of these new and complex challenges? A President Biden health reform package will likely include expansion of health care teams, exponential growth of telemedicine, and increasing dependence on reliable information to advance personal health planning.
Today’s modern health professionals are tomorrow’s health journalists. What principles should guide them in their new and expanded role. As a guide, I offer the following:
Continue reading…Value-based care – no progress since 1997?

Humana is out with a report saying that its Medicare Advantage members who are covered by value-based care (VBC) arrangements do better and cost less than either their Medicare Advantage members who aren’t or people in regular Medicare FFS. To us wonks this is motherhood, apple pie, etc, particularly as proportionately Humana is the insurer that relies the most on Medicare Advantage for its business and has one of the larger publicity machines behind its innovation group. Not to mention Humana has decent slugs of ownership of at-home doctors group Heal and the now publicly-traded capitated medical group Oak Street Health.
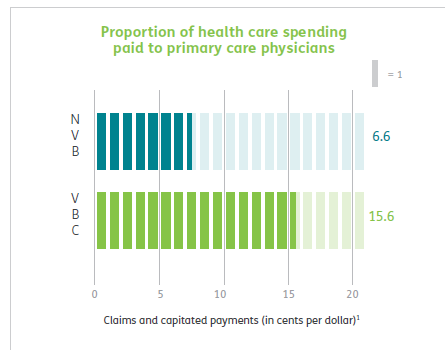
Humana has 4m Medicare advantage members with ~2/3rds of those in value-based care arrangements. The report has lots of data about how Humana makes everything better for those Medicare Advantage members and how VBC shows slightly better outcomes at a lower cost. But that wasn’t really what caught my eye. What did was their chart about how they pay their physicians/medical group

What it says on the surface is that of their Medicare Advantage members, 67% are in VBC arrangements. But that covers a wide range of different payment schemes. The 67% VBC schemes include:
- Global capitation for everything 19%
- Global cap for everything but not drugs 5%
- FFS + care coordination payment + some shared savings 7%
- FFS + some share savings 36%
- FFS + some bonus 19%
- FFS only 14%
What Humana doesn’t say is how much risk the middle group is at. Those are the 7% of PCP groups being paid “FFS + care coordination payment + some shared savings” and the 36% getting “FFS + some share savings.” My guess is not much. So they could have been put in the non-VBC group. But the interesting thing is the results.
#Healthin2Point00, Episode 157 | The phrase is “Takeout Speculation”!
Today on Health in 2 Point 00, Jess and I gossip about the wild rumor that UnitedHealthcare is acquiring Amwell. On Episode 157, we discuss Lark raising $55 million in a Series C along with a deal with Anthem to be their preferred DPP provider, Medicare Advantage plan Clover going public with a valuation of $3.7 billion, NOCD raising $12 million in a Series A providing specialized CBT and virtual OCD treatment, Cerebral raising $35 million in a Series A for its comprehensive digital mental health offerings, and Express Scripts adding to their digital health formulary with offerings targeting things like women’s health, tobacco cessation, muscle and joint pain, and more. —Matthew Holt
How Can Patients Get Medical Records from a Closed Medical Practice?
By GRACE CORDOVANO, DEVEN McGRAW, and AARON MIRI



The HIPAA Privacy Rule gives patients the right to copies of their medical records, with rare exceptions. When patients need a copy of their medical records, most start the process by calling their doctor’s office and asking for how to get access. The receptionist or office staff point them in the right direction, whether it’s instructing them to write down their request and sending it to the office, pointing them to contact the medical records or radiology department (if the practice is large enough), or assisting them in setting up their patient portal, if the practice is using an electronic health record (EHR). Being able to connect with a person inside the four walls of medicine is often crucial for many patients and their carepartners who may be unsure of exactly how to request their records.
But what happens to those records when a doctor closes or leaves the practice?
Independent practices close for a variety of reasons. Physicians may merge with a large practice or health system, retire, they may sell or close their practice for personal reasons, they may file for bankruptcy, or they may get sick and die. The COVID19 pandemic has had devastating financial consequences on many small, independent, and rural practices, leading to their consequent closure, acquisition, or merger.
What should patients do when their doctor’s office closes, and they need a copy of their medical records? This is especially challenging when a doctor may not have had an EHR, as is the case with many independent practices as well as more rural settings. On September 26, 2020, a tweet from Cait DesRoches, Executive Director of OpenNotes, inquired about how a family member may get access to medical records from her physican’s practice that closed, triggering a robust conversation that led to the realization that patients and families are not well informed in these circumstances.
Prevention is Worth a Pound of Cure
It can be much more difficult to get copies of records after a practice has closed. Patients should get copies of their medical records as they are generated instead of waiting until they’re needed. HIPAA Privacy Rule guidance states that individuals can get digital copies of digital information (or even digital copies of records kept on paper, as long as the practice has a scanner). Companies are developing tools and services that enable individuals and their care partners to collect, use, and store health records. Request digital (or paper, if that is preferred) copies of blood work, imaging, discharge instructions, and corresponding reports before you leave the practice.
Continue reading…THCB Gang Episode 27, 10/8

Episode 27 of “The THCB Gang” was live-streamed on Thursday, October 8th! Watch it below!
Matthew Holt (@boltyboy) was joined by some of our regulars: health futurist Ian Morrison (@seccurve), WTF Health Host Jessica DaMassa (@jessdamassa), writer Kim Bellard (@kimbbellard), patient & entrepreneur Robin Farmanfarmaian (@Robinff3), health economist Jane Sarasohn-Kahn (@healthythinker), and fierce patient activist Casey Quinlan (@MightyCasey)! We covered the recent presidential & vice-presidential debates, Trump on steroids, what the future of the ACA looks like, how will virtual care change public health, and more.
If you’d rather listen to the episode, the audio is preserved as a weekly podcast available on our iTunes & Spotify channels — Zoya Khan (@zoykskhan)
Will AI-Based Automation Replace Basic Primary Care? Should It?
By KEN TERRY

In a recent podcast about the future of telehealth, Lyle Berkowitz, MD, a technology consultant, entrepreneur, and professor at Northwestern University’s Feinberg School of Medicine, confidently predicted that, because of telehealth and clinical automation, “In 10-20 years, we won’t need primary care physicians [for routine care]. The remaining PCPs will specialize in caring for complicated patients. Other than that, if people need care, they’ll go to NPs or PAs or receive automated care with the help of AI.”
Berkowitz isn’t the first to make this kind of prediction. Back in 2013, when mobile health was just starting to take hold, a trio of experts from the Scripps Translational Science Institute—Eric Topol, MD, Steven R. Steinhubl, MD, and Evan D. Muse, MD—wrote a JAMA Commentary arguing that, because of mHealth, physicians would eventually see patients far less often for minor acute problems and follow-up visits than they did then.
Many acute conditions diagnosed and treated in ambulatory care offices, they argued, could be addressed through novel technologies. For example, otitis media might be diagnosed using a smartphone-based otoscope, and urinary tract infections might be assessed using at-home urinalysis. Remote monitoring with digital blood pressure cuffs could be used to improve blood pressure control, so that patients would only have to visit their physicians occasionally.
Continue reading…Attention, Walmart Patients
By KIM BELLARD

When Walmart announced earlier this summer that it was opening an insurance agency to sell Medicare-related products and services plans, I thought, “that’s it?” When Walmart announced later in the summer that it was partnering (first with Microsoft, then with Oracle) in the bid to buy TikTok, I thought, “well, isn’t that interesting?” And when Walmart announced a few days ago that it was partnering with Clover Health to offer Medicare Advantage plans, I thought: “it’s about time.”
You know Walmart. 265 million people (worldwide) shop at its stores each week. Ninety percent of Americans live within 10 miles of a Walmart store. It is estimated that 95% of Americans shop at Walmart during the year. In over 200 U.S. markets, it accounts for at least 50% of grocery sales. It is the fifth largest pharmacy chain by revenue.
And Walmart has been shaking up healthcare for some time. Way back in 2006, it introduced its $4 Prescriptions program that upended pharmacy pricing. In 2008, it started offering in-store retail clinics, initially in partnership with hospitals and now operates on its own.
Continue reading…#Healthin2Point00, Episode 156 | Garage Sale Edition
Today on Health in 2 Point 00, Jess can’t figure out what’s going on with health tech investors. Episode 156 feels like rummaging through a garage sale… First up is mirrors, mirrors, mirrors, with a total of $225 million invested: Tonal gets $110 million, Tempo gets $60 million, and Fiture gets $65 million. Next up is socks; Siren, which makes socks, added $9 million to their B round, which already has $11 million. Our next category is doctors, aka startups from Europe with “doctor” in the name: DrDoctor gets £3 million in an A, HomeDoctor scored €3.7 million, and Your.MD gets $30 million. Finally, we have raccoons! Raccoon.World closes a $900 million seed round to provide physiotherapy in a video game platform. —Matthew Holt
New Technologies Drive Cost Growth Over Time
By KEN TERRY
(This is the eighth and final installment in a series of excerpts from Terry’s new book, Physician-Led Healthcare Reform: a New Approach to Medicare for All, published by the American Association for Physician Leadership.)
Medical technologies include drugs, devices, tests, and procedures. Considered as a whole, these technologies are the key driver of growth in health costs, according to Georgetown University professor Gregg Bloche and his associates.
Bloche, et al., view insurance coverage as the chief enabler of these technological innovations. In a 2017 Health Affairs Blog post, they said, “Drug and device developers, clinical researchers, and their financial backers anticipate coverage for new tests and treatments with little concern for whether they add substantial therapeutic value, and they make research and development decisions accordingly.”
In an interview, Bloche further explained, “If you’re a technology developer, you can reasonably anticipate that if your product achieves a low but significant health gain, insurers are going to be under pressure to pay for it.”
Insurers do cover most new drugs, although they may make it difficult for patients to access the ones that they deem to be low-value, notes Peter Neumann, director of the Center for the Evaluation of Value and Risk in Health at the Institute for Clinical Research and Health Policy Studies at Tufts Medical Center in Boston.
Continue reading…








