 2014 will see wide-scale production and exchange of Consolidated CDA documents among healthcare providers. Indeed, live production of C-CDAs is already underway for anyone using a Meaningful Use 2014 certified EHR.
2014 will see wide-scale production and exchange of Consolidated CDA documents among healthcare providers. Indeed, live production of C-CDAs is already underway for anyone using a Meaningful Use 2014 certified EHR.
C-CDA documents fuel several aspects of meaningful use, including transitions of care and patient-facing download and transmission.
This impending deluge of documents represents a huge potential for interoperability, but it also presents substantial technical challenges.
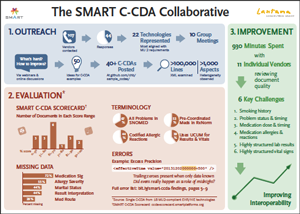
We forecast these challenges with unusual confidence because of what we learned during the SMART C-CDA Collaborative, an eight-month project conducted with 22 EHR and HIT vendors.
Our effort included analyzing vendor C-CDA documents, scoring them with a C-CDA scorecard tool we developed, and reviewing our results through customized one-on-one sessions with 11 of the vendors.
The problems we uncovered arose for a number of reasons, including:
- material ambiguities in the C-CDA specification
- accidental misinterpretations of the C-CDA specification
- lack of authoritative “best practice” examples for C-CDA generation










