Some measures of health care quality and patient safety should be taken with a grain of salt. A few need a spoonful.
In April, a team of Johns Hopkins researchers published an article examining how well a state of Maryland pay-for-performance program measure for dangerous blood clots identified cases that were potentially preventable. In reviewing the clinical records of 157 hospital patients deemed by the state program to have developed these clots — known as deep vein thrombosis and pulmonary embolism — they found that more than 40 percent had been misclassified. The vast majority of these patients had clots that were not truly preventable, such as those associated with central catheters, for which the efficacy of prophylaxis remains unproven.
These misclassified cases of blood clots resulted in potentially $200,000 in lost reimbursement from the state, which penalizes hospitals when the additional treatment costs related to more than 60 preventable harms exceeds established benchmarks.
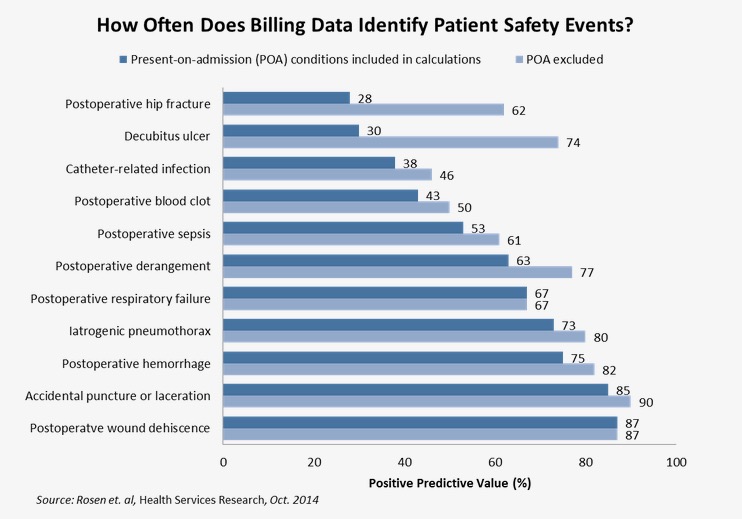
Why the discrepancies? The state identified cases of these clots using billing data, which utilize the diagnosis codes that medical billing specialists enter on claims. These data, also known as administrative data, lack the detail that would be available in the actual clinical record, considered by many to be the most trusted source for safety and quality measures.







