The paper is from Leonard et al and it’s published in PLoS ONE, so it’s open access if you want to take a peek. The authors used a database system in the state of Western Australia which allowed them to find out what happened to all of the babies born between 1984 and 1999 who were still alive as of 2005. There were 400,000 of them.
The records included information on children diagnosed with either an autism spectrum disorder (ASD), intellectual disability aka mental retardation (ID), or both. They decided to only look at singleton births i.e. not twins or triplets.
In total, 1,179 of the kids had a diagnosis of ASD. That’s 0.3% or about 1 in 350, much lower than more recent estimates, but these more recent studies used very different methods. Just over 60% of these also had ID, which corresponds well to previous estimates.
There were about 4,500 cases of ID without ASD in the sample, a rate of just over 1%; the great majority of these (90%) had mild-to-moderate ID. They excluded an additional 800 kids with ID associated with a “known biomedical condition” like Down’s Syndrome.
So what did they find? Well, a whole bunch, and it’s all interesting. Bullet point time.
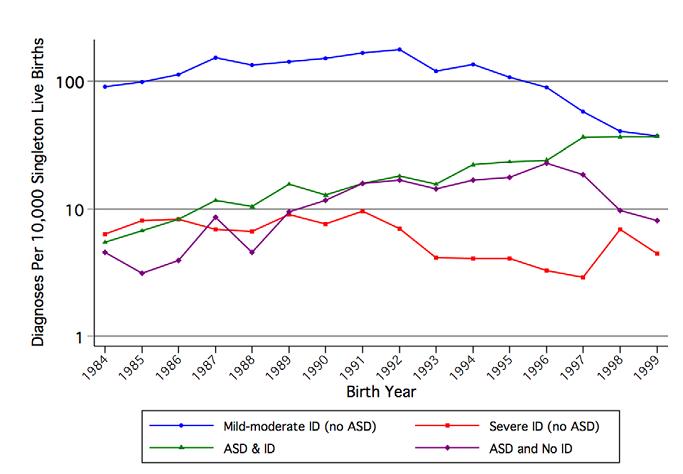
- Between 1984 to 1999, rates of ID without ASD fell and rates of ASD rose, although there was a curious sudden fall in the rates of ASD without ID just before the end of the study. In 1984, “mild-moderate ID” without autism was by far the most common diagnosis, with 10 times the rate of anything else. By 1999, it was exactly level with ASD+ID, and ASD without ID was close behind. Here’s the graph; note the logarithmic scale: