


By CHITRA CHHABRA KOHLI MD, AJAY KOHLI MD, and VINAY KOHLI MD, MBA
With a doubling time of cases estimated between 3 days within the U.S. and about 6 days globally (at the time of this writing) COVID-19 is demonstrating its terrifying virulence as it spreads across the world.
What’s perhaps equally terrifying, if not more, is the absence of a known cure or treatment plan for COVID-19. While there has been a lot of attention focused on Hydroxychloroquine and Azithromycin, there has been debate on the scientific validity of these treatment options, either as therapy or as prophylaxis. The impact of a solution certainly has far reaching potential, the scope of the challenge is overwhelmingly large. The editor-in-chief of Science recently wrote that the efforts to find a cure are not just ”fixing a plane while it’s flying — it’s fixing a plane that’s flying while its blueprints are still being drawn.”
There is a promising therapy that may help us weather the COVID-19 storm and, perhaps, flatten the curve. It’s based around science that defines immunology and has already been used in many different diseases, going as far back as the 1918 flu pandemic. This potential treatment is convalescent plasma therapy — using antibodies from patients who have recovered from COVID-19 and then transfusing them into patients who are currently mounting an immune response against the rapidly rising viral loads of COVID-19.
How COVID-19 Attacks
To understand how convalescent plasma therapy, or really how any therapy can play a role in treatment, we need to understand how the disease, COVID-19, attacks.
COVID-19 is transmitted through direct and indirect human-to-human contact, with community spread increasing everyday. The R0 (pronounced R nought) of COVID-19 is estimated around 2.2 (movie star Kate Winslet simplifies this complex epidemiological concept in less than a minute and a half, in this brilliant scene from the movie Contagion, included here). Among the many sinister qualities of the virus is its patience — it has an incubation period which can last up to 14 days — making it particularly virulent because of its ability to be spread unsuspectingly. Clinically, it presents often with fever, dry cough, shortness of breath and other respiratory symptoms, although it’s reported in a not insignificant minority to also present with gastrointestinal complaints.
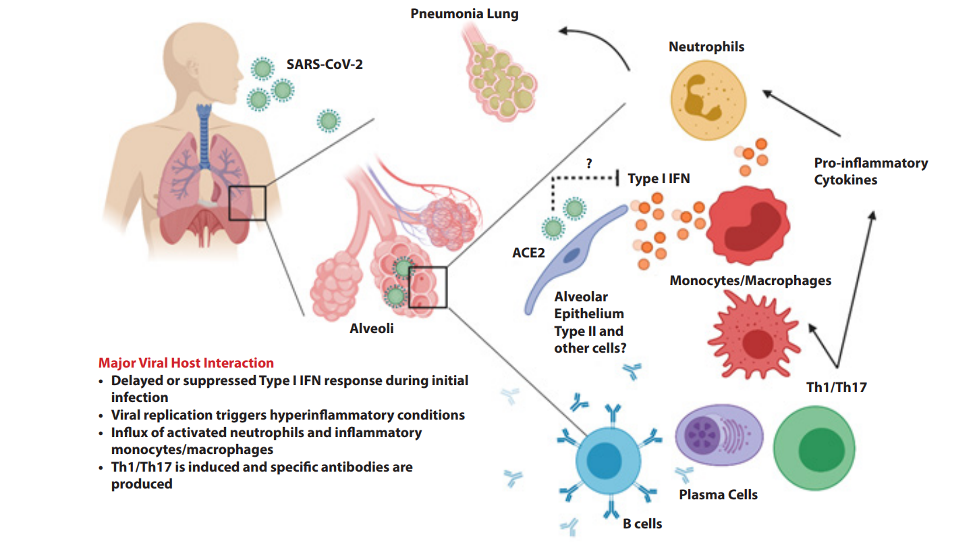
After the initial symptomatic presentation it begins to unleash its full force, manifested through a cytokine storm.
The body’s immune system is a complex army used to defend against the attacks of invaders, like COVID-19. Cytokines — small proteins that unleash a pro-inflammatory fight against invaders — are typically balanced by a legion of lymphocytes, cells responsible for clearing out inflammation. When COVID-19 invades its host it unleashes an unfair war — causing a toxic cytokine storm with lymphopenia (a reduction in the number of lymphocytes) — leaving the body susceptible to an unchecked inflammatory state. This can go on to cause lung injury, leading to acute respiratory distress syndrome, shock, organ failure and potentially death.
This is what was seen within the original cohort of patients from Wuhan who all had increased IL-6 (an inflammatory cytokine) and other markers of inflammation (increased neutrophils and C-Reactive Proteins) with decreased lymphocytes. Furthermore, these patients with increased neutrophils and decreased lymphocytes were sadly shown to have a higher rate of disease severity and death.
It’s a battle between the multiplying COVID-19 viral load and the body’s immune system. However, even before the battle begins, COVID-19 causes a decrease in the lymphocyte count, essentially destroying the armor of the immune system. With an unchecked increase in viral count, and a hobbled immune system, the lungs, are the early casualty in the war.
Role of Plasma
As the virus count increases within the body, there are progressively higher rates of inflammation with decreased lymphocytes to clear this inflammation. Could patients be administered therapy in this critical time to help bolster their immune system against this virus?
In limiting the increase in viral load count, convalescent plasma therapy could do precisely this. While this has already been used with H5N1 avian influenza and H1N1 influenza, and there has been at least one study in patients with COVID at the Shenzen Third People’s Hospital in China. Their efforts showed that critically ill patients with COVID-19 improved on multiple different parameters after the administration of plasma therapy.
Their study selected patients who were previously diagnosed with COVID-19 in the past, but had negative viral loads of SARS-CoV-2 (the causative agent for COVID-19) at the time of blood donation. Additionally, the donors were required to be asymptomatic for at least 10 days with serum SARS-CoV-2–specific ELISA antibody titer greater than 1:1000 as well as a neutralizing antibody titer greater than 40 (similar parameters to the administration of plasma therapy in prior pandemics, such as H1N1). After blood donation, 400 mL of convalescent plasma was obtained from each donor by apheresis, with the plasma immediately transfused to critically sick recipients on the day it was obtained.
The plasma recipients showed a very promising response — including decreased viral loads, improved PaO2/FiO2 as well as decreased body temperature and time to discharge (see figure below). Promisingly, these responses were similar to the patients who had been administered convalescent plasma therapy in other diseases.

So why did these critically ill patients who were all receiving potent antivirals without improvement suddenly get better? The answer lies in the ability to control the viral load. Prior to the administration of convalescent plasma therapy, the patients were all being treated with potent antivirals but their viral loads were still detectable and rising. After the administration of plasma therapy, their viral loads declined to undetectable levels. In the setting of a reduced viral load, the patients were able to compound acceleration of infected cell clearance.
What is plasma? Plasma makes up 55% of the body’s total blood volume and contains a variety of important proteins — most notably antibodies. In simplified terms, antibodies essentially are ‘memory’ proteins that become primed to detect ‘invaders’ after a host becomes exposed — either through infection or vaccine. Antibodies allow hosts to not only better detect ‘invaders’ and clear them out of body, but also improve the efficiency and efficacy of the immune system to clear ‘invaders’ out quickly, thereby minimizing disease progression and severity. It is this principle — ‘priming the immune system’ — that underlies the use of vaccines.
The study performed at the Shenzen Third People’s Hospital in China was limited because it was only performed in 5 patients. However, convalescent plasma therapy has shown promise through numerous prior pandemics. The risks and benefits of convalescent plasma therapy are well known, although work still has to be done to evaluate it further, particularly within the setting of COVID-19.
Implementation
It must be stated that is not the cure for all.
The FDA has already released plasma therapy as an emergency Investigational New Drug Application (eIND) for use in patients with serious or immediately life threatening emergencies. The FDA did add, however, that clinical trials still have to be performed to determine the safety and efficacy of plasma therapy before administering plasma therapy routinely. In the absence of options, this could be used for critically ill patients that are unable to mount a response to the disease.
Mount Sinai in New York City has already started administering antibody rich plasma therapy for the most critically ill patients. Additional healthcare institutions are already looking at starting clinical trials while nearly every major US academic center is looking to expand their treatment options with convalescent plasma therapy.
Perhaps the most comprehensive resource is the National COVID-19 Convalescent Plasma Project – https://ccpp19.org/. Based out of Mayo Clinic, this website serves as a resource for healthcare providers who are looking to use plasma therapy for either clinical trials or treatment. This also serves as a platform for patients who have recovered from COVID-19 to donate their plasma or for patients/family members considering the treatment.
Diagnostics
The power of the immune system is currently being harnessed as the race for a vaccine begins. However, while we wait for a vaccine, mapping the antibody response can be critical in the development of new tests.
Abbott Laboratories recently launched a molecular point of care swab test that has received Emergency Use Authorization (EUA) by the FDA to detect viral loads within a short period of time. This test utilizes RT-PCR (Reverse Transcriptase – Polymerase Chain Reaction) to determine if a sample is positive within 5 minutes and negative within 13 minutes.
There is an additional rapid COVID-19 IgG/IgM antibody blood test. This test had already been deployed in China, where it had high sensitivity (88.66%) and specificity (90.63%). This could be most useful in preventing asymptomatic spread where patients can test false negative by swab PCR, particularly in the early stages of infection. COVID-19 spread is estimated to start within the lungs and may not show up in the early phase with a swab test, leading to a false negative result.
This could be particularly useful in filling the void of testing asymptomatic carriers of COVID-19, with a false negative RT-PCR, and then placing them in quarantine. This is not unique to COVID-19, as patients with Zika demonstrated to be asymptomatic carriers as well. While the window to implement this may be missed within New York City, there could be a potential role in areas where COVID-19 has yet to spread and surge.
Future steps
As the number of patients with COVID-19 increases, resources – from ventilators for the patients to personal protective equipment for the providers – are already being strained. This is another area where convalescent plasma therapy could play a role. With variations in underlying baseline immunocompetence, it is inevitable that patients will either recover or worsen. Those that recover could potentially hold a life-saving treatment that could save the most critically affected or perhaps even prevent the deteriorating patient from becoming critically ill.
In the absence of a cure, and in the long wait for a vaccine, convalescent plasma therapy is a solution that could give a suffocating world a much needed breath of fresh air.
Dr. Chitra Chhabra Kohli is Medical Director and Consultant Surgical Pathologist at Coffeyville Regional Medical Centre, Coffeyville, Kansas.
Dr. Vinay Kohli is an independent pathologist and former Professor from the Department of Pathology, King George’s Medical University, India.
Dr. Ajay Kohli is a radiology resident physician at the Hospital of the University of Pennsylvania in Philadelphia, PA.
Categories: Uncategorized







