 The U.S. tax system and health care are deeply intertwined. The Republican tax bills hurtling through Congress would make significant changes in this relationship.
The U.S. tax system and health care are deeply intertwined. The Republican tax bills hurtling through Congress would make significant changes in this relationship.
The proposed changes, primarily a large cut in the corporate tax rate from 35 to 20 percent, would benefit health care (and most other) companies.
But none of the changes would, in the long run, benefit consumers, the public good, or public health. The major components of the proposed legislation are dangerously ill-conceived and ill-timed in the context of the overall economy and in particular health care policy and spending, which is projected to comprise 20 percent of the nation’s economy in 2025, up from 18.3 percent today.
That’s a difference and increase that reflects several trillion dollars of “additional” health care spending over the next decade. Amid this projected rise, the Trump administration and congressional Republicans propose to reduce the rate of growth of overall federal government spending and shift a sizable portion of health spending to other government entities and programs. These include the Pentagon, national security, homeland security, infrastructure projects, and—most notable in the context of the tax bills—a tax cut for corporations and upper income Americans.
It doesn’t and won’t add up—unless two (unlikely) things happen: (1) the economy grows at twice to three times the rate most economists predict and (2) the rate of growth in health spending is dramatically constrained.
Absent both, the Republican tax bills will cause the annual federal budget deficit and the nation’s long-term debt to balloon even more than already forecast.
This outcome is highly irresponsible and could lead to adverse economic consequences, especially in the event of a major war, terrorist attack, natural disaster (such as a pandemic) or weather/climate-change-related event.
In addition, over the long run, excessive deficits and debt are a tax and dangerous burden on our children and grandchildren during a period in which fewer workers will be subsidizing a growing number of senior citizens.
What follows is Part 1 of a series of pieces on the Republican tax legislation’s health care components. This piece deals with the federal budget deficit, national debt, and projected health spending. Part 2 will discuss the proposed elimination of the individual mandate to purchase insurance under the ACA—if that proposal remains in the proposed legislation. As of this writing, it’s in the Senate tax bill but not the House bill. The White House and Republicans have sent mixed signals on the fate of the mandate over the past two weeks.
Deficit spending, debt and health care
As has been widely reported, the tax legislation would add an estimated $1.5 trillion to the national debt over the next decade (some analyses show it closer to $2.2 trillion). Republicans dismiss this as a trivial amount and say economic growth, spurred primarily by the corporate tax cut, will more than make up for it.
Many independent and Democratic-affiliated analysts disagree. They argue that (1) there’s no proof the corporate tax cut will add more than a fraction (less than 1%) to economic growth over the next decade, and (2) that an increase in deficit spending, and thus the national debt, at this point is greatly at odds with the current debt load, national priorities, overall projected government expenditures, and the government’s commitments to provide health insurance and care to upwards of 120 million Americans.
The national debt is currently $20 trillion. That’s more than triple the debt in 2000, when it was $6 trillion. Federal government spending (our tax dollars!) to pay the interest on that debt varies from year to year. It mostly trends between 5 and 10 percent of the federal budget each year. In 2017 it was 6.5 percent. In 2018 it will be 8 percent—$315 billion of a $4 trillion federal budget.
For a host of reasons, interest on the national debt is projected to be the fastest growing federal expense over the next decade. It’s projected to rise every year over the next decade to $787 billion by 2026 and in that year comprise 12.2 percent of the federal budget.
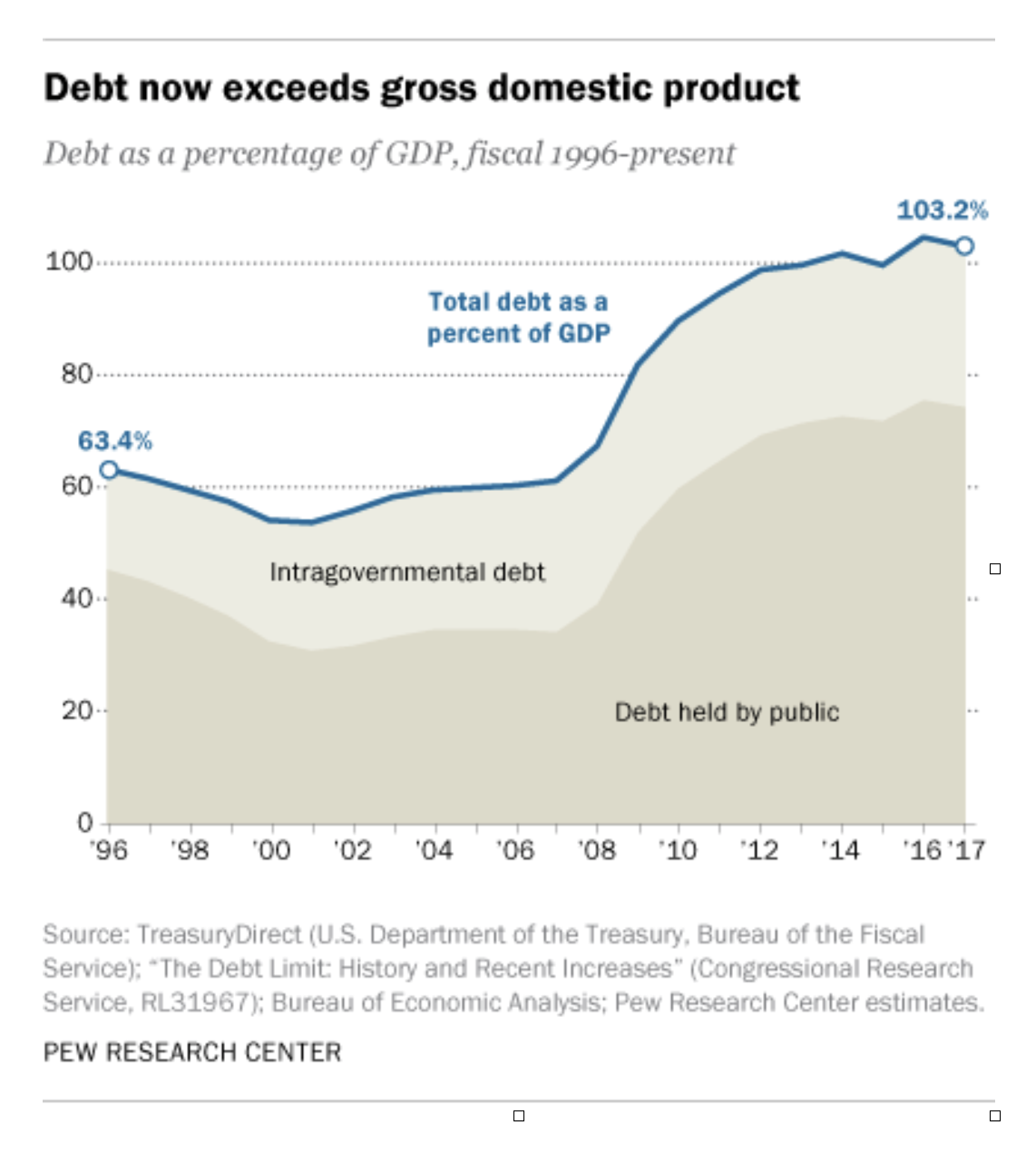
Economists track the national debt in another way, too: as a percentage of overall GDP. That’s considered a more robust and meaningful measure for technical reasons. The table below indicates what many observers believe is a very precarious situation: our nation’s debt is now at around 100 percent of GDP. The GDP was $19.4 trillion in 2017.
The only other time it was that high was during and right after World War II.
And deficits and the debt are poised to rise further. If current tax receipts and federal expenditures, including for health care, were to continue at a pace equal to the past few years (often referred to as the baseline), CBO forecasts a federal budget deficit of close to $1 trillion in 2024.
In CBO’s words: “The projected rise in deficits would be the result of rapid growth in spending for federal retirement and health care programs targeted to older people and to rising interest payments on the government’s debt, accompanied by only moderate growth in revenue collections. Those accumulating deficits would drive up debt held by the public from its already high level to its highest percentage of gross domestic product (GDP) since shortly after World War II.”
As is well known by health policy folks, Medicare and Medicaid account for bulk of health spending by the federal government (again, our tax dollars). And there’s no let up in sight.
As most recently projected by CMS’s Office of the Actuary, Medicare spending will increase between 7.1 and 7.6 percent annually from 2019 to 2025. That program alone will make up 18.8 percent of the federal budget in 2019 rising to 21.4 percent in 2025.
Medicaid spending is projected to increase around 6 percent a year between 2019 and 2025, and make up 9.2 percent of federal government spending in 2019 and 9.5 percent in 2025.
Other tax-supported health care spending is also forecast to rise, including for the VA and active military, CHIP, tax dollars devoted to federal employees’ health insurance, and subsidies/tax credits for people who enroll in the ACA exchanges.
CBO issued a report in September taking stock of several of these avenues of expenditures over the next decade—again, as a baseline assessment not factoring in any change in law.
The tax exclusion for employer-based coverage (which, by the way, is among the largest tax breaks in the current tax code) will “cost” the government $297 billion in 2018, rising to $475 billion in 2027. Cumulative cost 2018-2027: $3.8 trillion.
As an aside, the idea of limiting this exclusion has been debated for years since it is regressive; it benefits upper-income people far more than lower-income because upper-income people have, on average, richer benefits. It benefits people who buy coverage on their own and the uninsured not at all. A cap on the exclusion at a certain actuarial level could save between $50 and $100 billion a year. But that is politically unlikely to happen for the foreseeable future.
Tax credits for those who purchase coverage in the ACA exchanges will cost the government $41 billion in 2018, rising to $62 billion in 2027. Cumulative cost 2018-2027: $531 billion.
Medicaid coverage triggered by the ACA’s Medicaid expansion will cost the government $76 billion in 2018, rising to $143 billion in 2027. Cumulative cost 2018-2027: $1 trillion
There are other commitments and costs as well, such as for CHIP (cumulative 2018-2027 spending: $64 billion) and the cost-sharing reduction payments (cumulative over the next decade: $99 billion, if those payments get restored in Congress as expected).
All totaled, the tax benefits in existing law plus commitments and expenditures under the ACA for added coverage for the non-Medicare population add up to $654 billion in 2018. That is forecast to rise to just over $1 trillion in 2027. The cumulative cost 2018 to 2027: $8.2 trillion.
And don’t forget: 30 million Americans under age 65 are expected to remain uninsured each year over the next decade. If we choose as a society to extend coverage further—via Medicaid, the ACA exchanges or new programs—where does the money come from?
Conclusion
The U.S. spends a whooping amount on health care—across the board. Its’ commitments in this area of the economy are huge. Health spending is forecast to rise at a rapid clip over the next decade. Without substantial changes in the way we pay for health care that leads to a reduction in the rate of increase, rising expenditures are unavoidable and become unsustainable if other societal needs are to be met.
Tax cuts and reforms that add to deficit spending and seek to reduce health care spending growth by (a) slashing budgets, (b) eliminating coverage or benefits and/or (c) shifting costs to consumers—without making major structural changes in the way we pay for care and how much we pay—are a dereliction of fiduciary duty.
In this context, the Republican tax bills and the Trump administration’s 2018 budget are bad law and bad policy and should be rejected.
Categories: Uncategorized








Here is a little dose of perspective:
The CBO analysis that comes up with 1.5T debt increase over ten years assumes GDP growth of 1.9%.
If GDP growth is 2.6% the tax plan will be revenue neutral….no addition to debt.
If GDP growth is greater than 2.6% the national debt will go down.
Current run rate of GDP growth is over 3%.
During the Obama administration the national debt grew by an average of 1 trillion per year, cumulative 10 trillion.
The apocalyptic predictions are a bit overdone.
Furthermore, there is no reasonable basis to assume that our current, diffusely focused level of healthcare reform will do anything to improve its cost and quality problems. Recently, there has been an increasing support for implementing a single payer as the best solution for the cost and quality problems of our nation’s healthcare. The rush to this solution ignores the likely need for draconian rationing that would be required to improve its efficiency. Also, the single payer concept would not necessary achieve mitigation of the social adversities that drive a large portion of the cost and quality problems: smoking, obesity, poverty and dysfunctional family neighborhoods.
.
Henry J. Aaron, Ph.D. is an economist at the Brookings Institute. He wrote a Commentary for the NEJM published in 2010. I quote a portion of it:
“Current projections indicate that government debt owed to the public will reach 90% of national output in 2021, a decade from now. There is nothing magic about this number, but many observers fear that if the debt reaches that level and is headed higher, savers here and abroad will come to doubt the capacity and willingness of the United States to service its debt. Should such a loss of faith occur, the interest rate that the government – and borrowers – would have to pay would soar. Rising interest rates would multiply the debt burden, simultaneously aggravating the government’s fiscal problems and discouraging private investment and consumption. Such a panic would be catastrophic.”
His comments bring to mind the recent affairs within Greece and Venezuela. Henry Aaron has been, and still remains, our nation’s economic expert regarding the financial issues of our Federal entitlement obligations, especially its ‘health spending.’
.
The steady increase in the portion of our national economy allocated to health spending has increased since 1960 at the rate predicted by Parkinson’s Law. There is absolutely no basis to assume that ANY current healthcare reform strategy will change the continuing increase in health spending as a portion of the Gross Domestic Product (GDP). There are defined and validated Design Principles for managing a Common Pool Resource (CPR). They were initially identified more that 10 years ago by Professor Elinor Ostrom, 2009 Nobel Prize winner. Current examples of a CPR problem can be noted by the preservation of *) the water level of the Republican River in Southwest Nebraska and *) the fresh water level in the aquifer under Los Angeles, CA. Also, the Cooperative Extension Service for our nation’s agriculture industry was established by Congress in 1914. Please note: our agriculture industry is the most efficient and effective for nutrition among the OECD nations, AND our healthcare industry is the least efficient and effective among these 35 nations of the world.
.
OK, everybody hold hands and take a deep breath, then say “It time for a Paradigm Shift” and finally, it you’re courageous, find http://www.nationalhealthusa.net/home/ for one proposal!