 If concepts could get awards, then “risk factor” would surely be a Nobel prize winner. Barely over 50 years of age, it enjoys such an important place in medicine that I suspect most of us doctors could hardly imagine practicing without it. Yet, clearly, the concept is not native to our profession nor is its success entirely justified.
If concepts could get awards, then “risk factor” would surely be a Nobel prize winner. Barely over 50 years of age, it enjoys such an important place in medicine that I suspect most of us doctors could hardly imagine practicing without it. Yet, clearly, the concept is not native to our profession nor is its success entirely justified.
A few years ago, on the occasion of the risk factor’s fiftieth anniversary, my colleague Herb Fred and I published an editorial highlighting some of the problem with the use of this concept. I will summarize here some of those points.
The risk factor concept was developed in the first decades of the twentieth century from within the life insurance industry as it began to systematically apply statistical methods in order to optimize actuarial predictions. The idea was to identify which baseline characteristics held by individuals would correlate with future risk of death.
The Framingham investigators imported this idea into the public health sphere and introduced the term risk factor in the medical literature in 1961. From then on, the concept and term have enjoyed an unmitigated success.
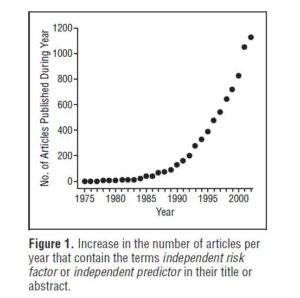
Originally confined to the cardiovascular arena, the concept is now thriving in every single medical discipline. The diagram below is from a 2005 paper by Brotman et al. The authors found that close to 1,200 papers per year claim new knowledge about “independent” risk factors. In the field of cardiovascular medicine alone, 105 such risk factors have been identified.
Furthermore:
–Risk factors, which can only make statistical claims, have morphed into full-fledged diseases. For example, hypercholesterolemia is not a naturally identifiable entity but a construct established by fiat on the basis of arbitrarily chosen cut-off numbers. Yet its disease status is widely embraced and it is sanctioned by an ICD code.
–The “diseasification” of risk factors has potential to cause harm by virtue of the so-called labeling effect. For example, it is well established that the incidence of headaches can be increased simply by affixing a label of hypertension to a person. Work absenteeism is also higher after patients are told they have high cholesterol levels.
–Risk factors garner plenty of attention even if their potential contribution to clinical outcomes is minuscule. One example is hypertriglyceridemia, whose independent contribution to the risk of cardiac disease is still debated. Obesity also barely increases cardiovascular risk when considered in isolation, and it may even be preventive in certain situations. Such attention to trivial risk factors may benefit the public health sector and the pharmaceutical industry, but whether patients are actually served remains to be seen.
–The incidence of risk factors is further increased by the establishment of “pre” conditions such as pre-hypertension and pre-diabetes. New risk factors can also be concocted by combining other risk factors, e.g., the so-called metabolic syndrome. Many newcomers are “proto risk factors,” i.e., risk factors for risk factors. One example is “normal weight obesity,” which is a risk factor for the metabolic syndrome.
–Frequently, the relationship between risk factor and clinical outcome is not as straightforward as claimed. For example, fatality rates for stroke have been in steady decline since the beginning of the twentieth century, long before any mechanism was available to identify or reverse its related risk factors. Likewise, careful analysis of life insurance data shows that coronary mortality has been declining since the mid 1950’s, before risk factor prevalence started to fall. Some risk factors, like hypertension, may have a “U-shaped” relationship to outcomes.
–Finally, as we now know from randomized clinical trials, risk factor modification is itself risky, as demonstrated by the trials of clofibrate, hormone replacement therapy, torcetrapib, rosiglitazone, to name but a few examples.
Risk factors have become the principal justification for turning medical care into a public health activity. Using risk factor modification as a surrogate for quality of care, doctors are given incentives to treat patients according to statistical norms. As we have shown in the paper, there is sufficient ambiguity to warrant caution against the widespread use of such a powerful concept.
Categories: Uncategorized








Agree completely! Social/political/psychological analyses of the motivations and incentives of the bureaucrat class are not scientific….but worthy of analysis in my opinion. Why do they keep mandating and imposing things on an entire profession without evidence their ideas will work?…and by and large avoid any consequences? And these are smart, well educated people. It strikes me as fertile ground for exploration….but maybe that is just me.
“a common affliction of the elites….altruistic narcissism”
___
Yeah, that’ll probably be REALLY scientific.
Thank you, Paul. I look forward to reading your paper on the altruistic narcissism of the elites! 🙂
Michel
Thank you, William. I agree with you that hypertension should be considered a risk factor rather than a disease, unless specific signs and symptoms are apparent, and those will depend on other factors such as genetic makeup or perhaps additional environmental insults. Herb Fred and I commented about how hypertension should be considered in this editorial: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2929868/
Michel
Excellent contribution!
I especially liked the reference to the bad history: “risk factor modification is itself risky, as demonstrated by the trials of clofibrate, hormone replacement therapy, torcetrapib, rosiglitazone, to name but a few examples.”
Statins will eventually join the list….though it will take a while since it is so ingrained, produces such huge profits for pharma, and lets docs and their bureaucrat masters feel like they are doing good (I am toying with the idea of a common affliction of the elites….altruistic narcissism….more to come if I am disciplined enough to flush out the concept and get it on paper).
Very interesting concept. Thanks for the excellent discussion.
With 23,000 genes and at least as many proteins–some genes are translated into several proteins–we have the foundational ingrediants for thousands of phenotypes which are the groups of actual noticeable forms and styles of life we notice in people (and which we are crudely picking up and almost randomly putting in boxes we call risk factors.) The risk factors are therefore an unscientific subset of the various phenotypes. But we are getting better.
So, what I am trying to say is that hypertension, eg, might have 50 genes contributing to its many varieties and we can hardly say that these 50 genes acting in thousands of permutations are a definite risk factor for another phenotype, say aortic aneurysm, which might have 30 other genes associated with it (some of which may be part of the group of 50.)
Thus, hypertension is a risk factor for aortic aneurysm in the crudest buckshot sort of way.
We are still in the early days of medicine. That’s what makes our days so rich with discovery and excitement.