Boston Physician Atul Gawande wrote The Checklist Manifesto in 2009 stressing that medicine should adopt “pilot’s checklists” to ensure that operating room teams are “ready for takeoff” before a scalpel is ever opened.
Here’s the “Time Out” done among all OR team members before a case beings – it includes a list of staff participating in the timeout, the agreed upon procedure, the verification of consent, appropriately marked operative site, patient identity verification, and best practices for prophylaxis.

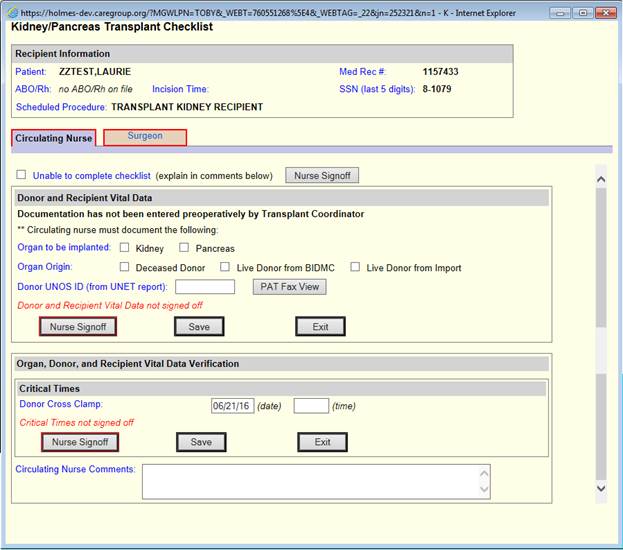
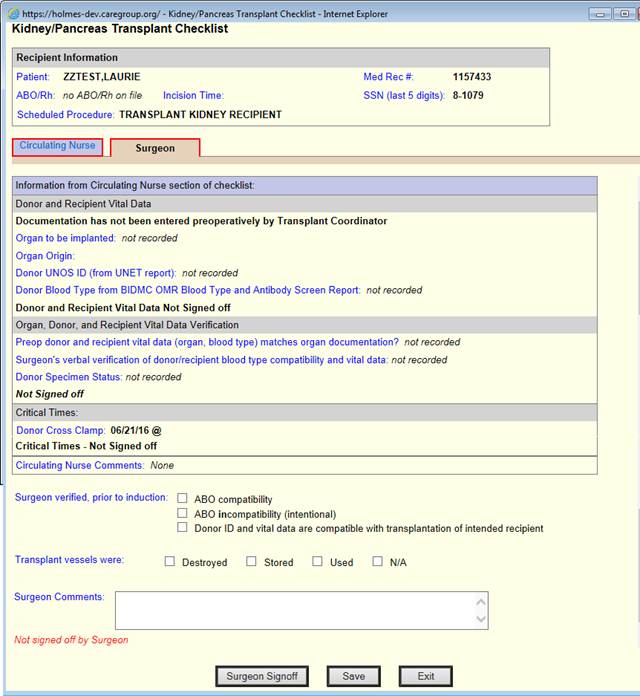
We also have procedure specific checklists for each operating room role. Here are transplant checklists for surgeons and nurses
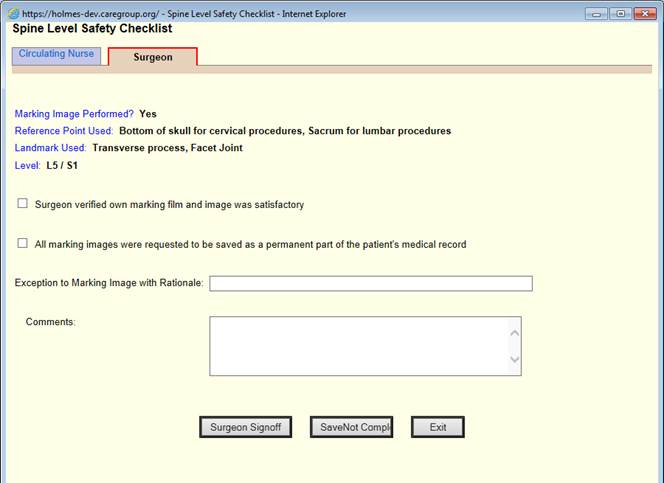
Here are spine surgery checklists for surgeons and nurses

Many complain that electronic health records create burden without significant benefit. Implementing checklists into the workflow of EHRs in the operating room is high value, ensuring good team communication, while also reducing error. A win/win for everyone!
John Halamka is the CIO of Beth Israel Deaconess Medical Center.
Categories: Uncategorized








Its a good article on highlighting the keypoints of EHR implementation.
I would also like to add a note that the historical data stored in the old EHR/EMR should not be forgotten. Many states require 5 to 7 years of data retention. Data management companies can help transition all the historical clinical and clinical data into the new EHR or archive them. There are some companies which specializes in such services – even without the cooperation of the old EHR vendor like https://www.triyam.com/data-conversion.html
Here is a link to my “List of features which should be in all EHRs” which was posted on The Health Care Blog
https://thehealthcareblog.com/blog/2016/06/09/features-which-should-be-in-most-emrsehrs/
https://thehealthcareblog.com/blog/2016/06/18/the-black-list-part-ii-features-which-should-be-in-every-ehr-but-for-some-reason-arent
Are the pilots checklists ALL computerized? Or are they pen and paper? IF the checklists are not made properly in a computer system or within a workflow of surgery, then they CAN be a mess and more unsafe. So you are a physician that uses computerized checklists in the office? In surgery? Please explain.
As a physician with a commercial pilot ticket, I can share that pilots who don’t use checklists during their exams don’t fly. I can also share that anytime there is an accident the FAA/NTSB looks to see if the checklist was used, if not “pilot error” is frequently the cause and the litigation frenzy ensues. Pilots have an added incentive to use checklists because they have ‘skin in the game’ too which is a slight but insignificant difference in the context of our oath to do no harm. Believe me, the studies have been done repeatedly by the FAA/NTSB, checklists work and pilots have complete buy in, at least those pilots among the living.
This has nothing to do with MACRA. Physicians who think they can ignore checklists because they are “computerized” or they are a “mess” should kiss their privilege to practice goodbye. Be grateful that someone is trying to keep you out of trouble.
This article is a great example of leveraging information systems to support the mission of the organization.
Here’s the thing…just because it “SOUNDS” like a good idea it is not always the case.
For surgery, the actual incidence of wrong site surgery went UP after sign the site and timeout was implemented. Yeah, see, sounds like a good idea. Look it up, its true.
So the “computerized” version of a “timeout” or checklist will not necessarily improve wrong site surgery nor problems, in fact, people will just click through the mess to get their day done. There NEEDS to be studies performed FIRST to see if this is not routinely ignored, worked around, needlessly impossible to use, causing other unintended consequences. JUST LIKE MU/MACRA, just because it sounds like a good idea to count clicks, check off quality indicators, it does NOT necessarily improve care, costs, safety or security, and certainly does not improve efficiency or usability.
SO JOHN H, I love ya, but before you say, “high value, ensuring good team communication, while also reducing error. A win/win for everyone!”
PROVE IT!