 Accountable care organizations (ACO’s) promise to save us. Dreamed up by Dartmouth’s Eliot Fisher in 2006, and signed into law as a part of the Patient Protection and Affordable Care Act (PPACA) in 2010, we have been sold on the idea that this particular incarnation of the HMO/Managed Care will save the government, save physicians and save patients all at the same time. I dare say that Brahma, Vishnu and Shiva together would struggle to accomplish those lofty goals. Regardless of the daunting task in front of them, the brave policy gods who see patients about as often as they see pink unicorns, chose to release the Kraken – I mean the ACO – onto an unsuspecting public based on the assumption that anything was better than letting those big, bad, test ordering, hospital admitting, brand name prescribing physicians from running amuck.
Accountable care organizations (ACO’s) promise to save us. Dreamed up by Dartmouth’s Eliot Fisher in 2006, and signed into law as a part of the Patient Protection and Affordable Care Act (PPACA) in 2010, we have been sold on the idea that this particular incarnation of the HMO/Managed Care will save the government, save physicians and save patients all at the same time. I dare say that Brahma, Vishnu and Shiva together would struggle to accomplish those lofty goals. Regardless of the daunting task in front of them, the brave policy gods who see patients about as often as they see pink unicorns, chose to release the Kraken – I mean the ACO – onto an unsuspecting public based on the assumption that anything was better than letting those big, bad, test ordering, hospital admitting, brand name prescribing physicians from running amuck.
I realize I am being somewhat harsh towards the creators of the ACO morass. But, while they all may be well-meaning, hard-working folks that own a Harvard crimson sweater, their intent is to fundamentally change how health care is provided – this mandates a withering evaluation. As Milton Friedman aptly said, “One of the great mistakes is to judge policies and programs by their intentions rather than their result.” Thus, with little regard to intent, and with an eye on the end result, I say unequivocally : ACO’s do not work.
I didn’t need big data to come to this conclusion. It came to me as I reviewed the details of an ACO commercial agreement that offered an extra $4 per patient per month for successful care coordination combined with the delivery of an as yet undefined high value care metric. The high priests that are only moved by mountains of evidence will look askance at statements like this because anecdotes like this have no real currency. The data, they preach, will cleanse, purify, and speak the truth. Small problem … the early results are in … and shocking no one who actually does care coordination, the results are not good.
Getting results on ACO’s is not easy – ask Kip Sullivan. Apparently, the smartest guys in the room who came up with ACO’s designed a construct that is so complex, assessing their effectiveness may require building a large hadron collider. The vehicle set in place by the ACA to provide for ACOs is the Medicare Shared Savings Program (MSSP). This program allows provider organizations (ACO’s) to share in savings with Medicare if spending is kept below a financial benchmark. The details of how the financial benchmarks are set up are somewhat opaque, but essentially amount to Medicare using a pre-ACO-contract-initiation period to arrive at a spending average baseline. Year over year changes in cost per beneficiary are then compared to the national average medicare spending growth. ACO’s that come in under the national average Medicare spending growth rate get to keep 50% of the savings that accrue to Medicare. Based on these benchmarks the Center for Medicare and Medicaid Services (CMS) announced last year that in 2014 ACO’s saved $411 million dollars.
There is, however, a significant problem with this approach. ACO’s are generally regional, and Medicare spending patterns vary widely by zipcode. It is not the best idea to compare ACO’s in regions with high cost growth to national spending growth patterns. A much more valid comparison would be to compare ACO costs with non-ACO costs within the same region. This is exactly what authors of a recent study in the NEJM attempted to do.
The authors looked at the medicare claims and enrollment database to calculate spending per medicare beneficiary by region in ACO patients and non-ACO patients. They examined ACO’s based on when they began (2012, or 2013), and looked at 2013 spending average data.
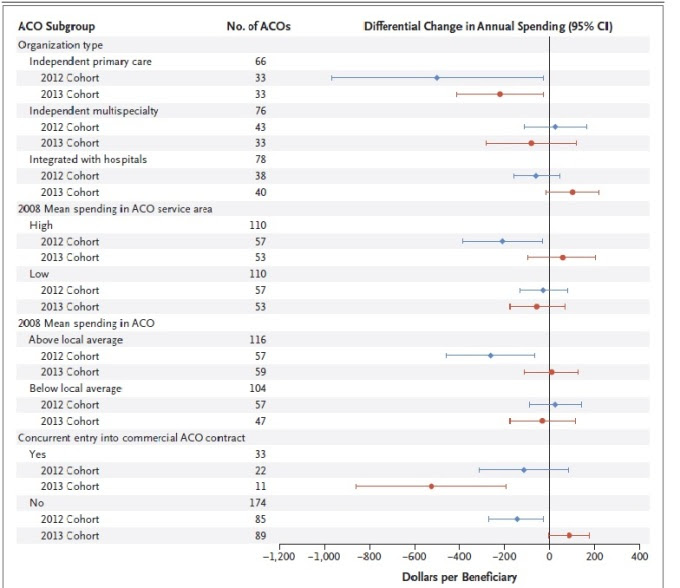
The grand total savings per beneficiary in the group of ACO’s that joined in 2012 was $144 (- 1.4%). ACO’s that joined in 2013 saved $3. To rub salt in the wounds, there was also no real difference seen in ‘high value’ care provided to patients (hospitalizations, 30 day readmissions). I hedged on the differences in high value care when I probably shouldn’t have – the ACO folks did get their LDL checked more often – yes, that was a metric of high quality care. The savings estimated for the 2012 ACO group was $238 million dollars, but unfortunately, there was no net savings because Medicare paid $244 million in bonuses to ACO’s. The study also gave no dollar value to the cost of setting up the ACO – one assumes someone is paying for that? The only silver lining I could find in the study was a subset analysis that showed significantly greater savings for independent primary care groups compared to groups integrated with hospitals.
To summarize:
- ACO’s that joined in 2012 demonstrated savings of $144/beneficiary
- ACO’s that joined in 2013 saved $3/beneficiary
- There was no meaningful difference in value delivered to patients within ACOs
- There were no net savings to Medicare after accounting for bonus payments paid to ACO’s
- ACO’s that consisted of primary care physicians saved significantly more money than groups integrated with hospitals
This early data should give policy makers pause. This was not a positive study, and it importantly re-enforces some significant concerns for physicians that are at the tip of the health care delivery spear. These concerns may be difficult to comprehend to the folks making decisions at one thousand feet… so allow me to take you to ground zero.
Ground Zero: The Story of Mrs. K
I received a message Saturday morning from my answering service. Mrs. K wanted to speak to me. I happen to be Mrs. K’s third cardiologist. I met her 2 weeks ago. She had gained 20 pounds over the last 3 months, had a kidney transplant, severe aortic stenosis and had a systolic blood pressure that stubbornly stayed above 200mmHg. She had shortness of breath just getting out of bed to go to the bathroom, and my fingers sunk in to her legs as if they were a memory foam mattress. It didn’t take me long to discover why I was her third cardiologist. She refused to listen to any of my suggestions, and went on to discount the reasonable suggestions of her prior cardiologists. She had a ‘reaction’ to almost every medication I suggested, and she decided on a daily basis if she would take the medicines that were prescribed to her. It took a combination of cajoling and threatening to finally have her trust me enough to come into the hospital. It took even more convincing – sometimes on a twice daily basis – in the hospital to get her to take the medications as prescribed. She improved markedly and was able to be discharged. Of course, this was just the start of our relationship. My office reached out almost every day to check her weights, and to re-enforce the need to take her medications. I called her back on Saturday, and listened, sometimes impatiently, while she relayed to me her feeling of chills that were definitely due to the pills I was administering. I tried to reassure her and implored her to stay the course.
I guess this is called care coordination. I just call it taking care of a patient. It is too early to know what will happen to Mrs. K. A hot dog’s worth of sodium may be enough to have her end up in the hospital again. Beyond the somewhat inconsequential debate about whether or not the patient would be attributed to me in a way that would allow me to share in some cost savings is the larger point that I could care less if Mrs. K was within an ACO or not. The ACO, in its current incarnation, does nothing to help me take care of Mrs. K. Those millions of dollars to the ACO’s? If your patient belongs to a hospital-run ACO, most of the Medicare cost savings do not end up with the physicians in charge of delivering high value care at a reduced cost. Let’s take my regional ACO – 30% of savings go to the ACO, 30% to those investing in the ACO (hospitals), and 40% to physicians. Any wonder that $4 per month is what’s left over after everyone has taken their cut?
I think the biggest sin the ACO’s commit is to distract from any real conversation about cost. There is plenty of cost savings to be had within the current construct, but we the public (Jim Purcell explores this well in his recent article) don’t want to make hard choices. We are a wealthy society, and a wealthy society prizes its health. In India, a rise in the price of onions is cause for rioting. In the great United States, suggesting mammograms not be covered until age 50 may result in charges of misogyny by liberals, and charges of fascist death panels by Palin republicans. Even the interventions that wouldn’t cost the public anything sit behind walls guarded by special interests. Currently, a significant pay differential exists between services provided by hospital-based outpatient departments (HOPD) and freestanding, physician-owned clinics. This means that the same echocardiogram provided in the same venue by the same people is many times more expensive if a hospital owns the clinic. This is not a secret. The Medicare Payment Advisory Commission (MEDPAC) has advised Medicare of this no-sense differential every year since 2012. Hospitals have resisted attempts to cut this vociferously, and successfully. But never you mind – just remember – the ACO will save us.
Anish Koka is a cardiologist based in Philadelphia.
Categories: Uncategorized








Steve, by rule the world – I meant that would be the prevailing thought of policy makers. I used to be in that camp – I have lost faith that the current folks in charge know what metrics to use and how to go about measuring this.
I don’t want to “rule the world”….I just want to apply a ruler (or other accurate measurement device) to what docs do. I stipulate in the blog that we are not yet doing that well, but it still must be done…because docs drive care and expenditure. They have to be accountable. MACRA is chance to make it all work better, including ACOs. Sorry, it’s not time to pull back. It’s time to up the ante, and get it right.
– Steve
Good thinking Anish,
I can’t believe they forgot the patient. The patient has to be a member of the ACO because it is he/she that is the subject of the effort, his cooperation that is needed, his consent that is needed before services are abridged or constrained, and his selecion of other participants and hospital for the team. They have all gotten together to try to make the patient better for less cost. He has to acceed to both the medical component and the cost component of this project. Therefore, he should benefit from some of the financial rewards too.
Relief to know you’re still alive .. I was going to send out a search party. Wonks do get away with saying the darndest things. Just read Steve findlays health affairs blog – the measure-measure-measure folks rule the world..
Read your piece. I agree – it is complicated. The ACO in its current form leaves much to desire. Your piece also reminds me that I’m no economist! Much to learn..
I’m not so sure about that Michael.. Medicare advantage per beneficiary – is more expensive to the fed govt. than traditional medicare.
https://thehealthcareblog.com/blog/2016/01/18/ask-not-what-you-can-do-for-medicare/
“I think the biggest sin the ACO’s commit is to distract from any real conversation about cost.”
What’s this! And bite the hand that feeds you.
“and ration care.”
Isn’t that what co-pays and HDHPs are supposed to do? Of course we need to ration care, but just for the other guy.
Good comments. As you say.. Doing care coordination sounds great but is expensive..I doubt the approach you describe will save money though I don’t have data to say that. As another commenter put it – the ACO attempts to model other successful integrated systems – but the secret sauce is missing :). Let me know when someone finds it.
My fellowship director will find this amusing, since I would vociferously argue for pilot programs to help bend the cost curve. He being a conservative warned about the shadowy central govt. taking control in a way that wouldn’t help doctors or patients. The last 8 years have proven him right and me wrong. These were not pilot programs – these were policy changes designed to take down fee for service, and the only way to really do that was to take away physician autonomy. The phrase Value based care was how they sold it. The reason they didn’t explain anything more was because they didn’t know any more.
Mr. Purcell makes one solid point here. When you’re unhappy with the status quo, change cannot be evidence-based, but aspiration-based. It can always, quite reasonably, be argued that change, such as an ACO, has not been given enough time to show its effect. Thus, the statement “ACOs may still deliver” cannot be negated. Since it cannot be negated it enjoys an enviable monopoly on evidence. It’s a bit like a coin toss: heads I win, tails you lose.
Nice piece Anish. I once asked a policy wonk why ACOs are going to be different from HMOs. His reply: “because we’re going to reward doctors for doing the right thing.” It was emblematic of the vacuousness that pervaded health policy circles peri-ACA.
As you mentioned, granularity is the Achille’s heel of measuring. I also remember the giddy days for the meme plague “measure, measure, measure.”
There’s a theme here ..
A complicated idea is developed by very smart people.
With little debate, the idea is pushed into service as policy and adopted on the national level. Unsurprisingly, considerable controversy ensues. Will the idea work? Is the investment in time and effort reasonable?
The architects are shocked and stung by the criticism.
After initial attempts to defend their experiments, they fall silent, charging their detractors with “just not getting it,” selfishness and other motives.
If there is one lesson we all should have learned by now, it is that major policy changes almost always require major implementation efforts. Complicated ideas need to be translated. Potential side effects need to be considered.
This has been the trend with almost all wonk-based policy in the past decade.
Wonks get algorithms, they get data, they get economics, they get acronyms, they get congressional hearings. On the other hand, they seem to not understand public relations and communication very well. Which is perhaps understandable.
After all, they’re wonks. They’re better with wonk to wonk communication and in situations where they’re viewed as experts, as is generally the case when they’re explaining their ideas to glassy-eyed politicians.
My mind is not yet made up about ACOs.
But I do know that in order for them to work they have to be sold. And in order to be sold, they need to be explained. In order to be explained, their architects must respond to inevitable questions and criticism.
This is as good place as any to start.
“The curious task of economics is to demonstrate to men how little they really know about what they imagine they can design.” F. A. Hayek. Excellent post, Anish
Barry, in my opinion, Medicare Advantage (“Medicare Part C”) has worked better than an ACO and is closer to the model you describe.
The politicians’ ideology is based on 2 premises: 1. The private sector….(for profit or non profit including docs)….cannot be trusted and 2. patients are too dumb and naive to be trusted. So the only solution has to be one run by government bureaucrats directing all aspects of medicine big and small….when ACO’s fail get ready for single payor….any alternative will be rejected out of hand.
The wonks (per John Irvine above): they share the above premises, but add the narcissistic element that THEY as the experts can design the right system….aka Hayek’s Fatal Conceit….not grasping that systems emerging as a consequence of millions of decentralized free choice decisions are much more intelligent and responsive.
Thanks Paul. It certainly is early. But as Kip Sullivan’s post 4 days ago on MACRA points out, I have little faith that anyone understands anything more than the intent of these policiies. The charge is to reduce payments in any way possible – the details to be figured out by the Wizard of Oz perhaps.
With regards to your second point – it is quite a reasonable alternative. Unfortunately the current administration appears married to the idea that dollars for health care no longer be treated tax free. Any thoughts on why they are so anxious to discredit this model?
Well put. I’m no expert either, and perhaps my delusion is believing that there are efficiencies to be had in the current marketplace. See my response below regarding coronary stents and interventional cardiologists. My hope is the smart guys go back to the drawing board – no signs of that happening yet.
Certainly true at the moment. Interesting that most of the programs that had ‘cost savings’ were in high cost regions. Would be interesting to see what happened in those programs – data of course is hard to come by.
I agree that ACO’s are a flawed concept. I happen to be in one. My wife and I have standard FFS Medicare plus a supplemental plan. We have the right to go to any provider we choose to that accepts Medicare whether they are part of the ACO or not. Last November I had an expensive cardiac procedure in a NYC academic medical center that is outside of my ACO. How can you hold an ACO doctor responsible for medical care he has no control over?
Also, defining and measuring quality in healthcare poses a whole separate set of challenges. Uwe Reinhardt suggests that healthcare quality can be divided into four parts which are (1) process – following evidence based protocols where they exist, (2) outcomes, preferably risk adjusted (somehow), (3) safety – minimizing infections, preventable readmissions, etc., and (4) patient satisfaction. All four would have to be measured and weighted. It’s a tall order to put it mildly.
I think we would be better served if we figured out how to pay doctors on a bundled payment basis to manage chronic diseases like CHF, CAD, COPD, diabetes, asthma, hypertension and depression which experts tell us account for about 75% of healthcare costs. We need a payment mechanism that allows doctors and their staff to have the flexibility to do what’s most appropriate for each patient including using nurse case managers to assess patient needs, remotely monitoring weight, heart rate, BP, glucose, etc., communication via phone and e-mail which don’t currently have billing codes in a fee for service system and reaching out to social service providers among other things. That array of services probably doesn’t come cheap but if it can minimize ER visits and hospital admissions, the potential savings are significant.
In the meantime, ACO’s are unlikely to work, in my opinion.
Thanks for the comments – and have to commend you on your great post that was eye opening and very informative.
The delusion I refer to is this idea that seems to now be ingrained in policy makers that shifting to outcomes based medicine by whatever 3 letter acronym you want is the answer. I, too, was a believer – it sounds great – but there are practicalities to this that relate to simply figuring out which outcomes to use that make this very challenging. Should we use blood pressure measurements as a quality metric? What target blood pressure should we use? The last five years has seen blood pressure targets change from lower is better, to lower is no better, to attempting to get lower is better. The American college of cardiology and the JNC 8 panel can’t agree on what blood pressure targets should be. Meanwhile, just today, I took a patient off of his blood pressure medications because he has at times extremely low blood pressures that have resulted in multiple hospitalizations. On paper – he’s a diabetic with heart failure on no blood pressure medications. We don’t have a system granular enough to do this – so why are we blindly barging ahead with outcomes based payment models?
Again, risk adjustment sounds good, but I routinely see patients with 20+ diagnoses in EHR’s. Hospitals have teams of people whose sole job is to scour hospital charts to find anything that will support a higher risk score. If you’re interested, the medicare advantage dalliance with risk is a fascinating read : https://thehealthcareblog.com/blog/2016/01/18/ask-not-what-you-can-do-for-medicare/
You suggest that it is the providers desire, or the culture of volume based medicine that is responsible for the early failure of the ACO… I would disagree. THere are certainly bad apples, but I don’t think most of my colleagues subscribe to this model. We are, in general, loathe to cause harm. As an example I give you coronary stenting…Since the COURAGE trial came out in 2007, elective coronary stenting has decreased 50%! Why did this happen? It wasn’t because of ACO’s – it was because of physician probity (I hope to develop this in another post). The system worked. Data came out suggesting little benefit for stenting over medical management – and the mass of interventional cardiologists working in a fee for service model significantly reduced stent placement.
Health care costs btw were flat at ~17% of GDP between 2009-2013. 2014 saw an uptick only because of the expanded coverage by the ACA.(http://thedoctorweighsin.com/healthcare-costs-are-on-the-rise-again/). .
So I wouldn’t say yes to your question on changing how we pay for health care delivery. I would hedge – there certainly are changes in how we must pay for healthcare (I discussed a simple one of them – reducing payments to hospital based practices for certain services delivered) – but the idea that the only way forwarded is some form of a bundled payment model is unsupported. As you brought out in your post, unless we have a real discussion of what the public is ok with giving up – I think these alternative payment models are bound to fail – and certain to make me lose large amounts of precious hair.
in 2012 I wrote an article entitled, “How a Flaw in the ACO Model Leaves Patients Out” http://www.govhealthit.com/news/how-flaw-aco-model-leaves-patients-out
While federal legislation focuses on payor / provider synergies, there is nothing in the mandated programs beyond pilot projects or experiments according to the legislative texts.
Milton Freedman and Dr. Koka are right.
Maybe some day, some how, ACO’s will prove to be great.
Many (most?) of the “anointed” health policy experts have all glammed on to the ACO idea.
Thankfully, we have Anish Koka and Kip Sullivan looking at what research has shown so far….it is not a pretty picture.
I hope ACO’s live up to the hype and they deserve a chance, as long as patients have the choice to sign up to ACO’s ….(with appropriate disclosures that they are volunteering to be subjects in an experiment) or to choose other kinds of networks But the anointed policy experts are dismissive of the notion that patients have any ability to sort things out, and dismissive of the call for careful research before we go “all in”. Vermont is trying to pass legislation and get Federal waivers to force everyone in Vermont into an ACO…
We do know that most savy employers have decided to offer high deductible plans linked to health savings accounts…and that employees like these plans. And we have sound research from Rand that shows they work in reducing cost/slowing medical inflation. http://www.rand.org/news/press/2011/03/25.html
GE reduced total medical expenditures 14% when they went to this model. (WSJ, September 2012). But everyone in health policy likes to ignore the fact that these plans work….unfortunately the Affordable Care Act offers Frankenstein versions of high deductible plans (without health savings accounts) that seem more oriented to discredit the model than allow it to work).
The old joke is that a camel is a horse designed by committee.
By the same token, ACOs were and are clumsy attempts to replicate the economies of scale and in-house efficiencies of a handful of systems that have been achieving good outcomes for years at fractional costs — compared with a multitude of providers paying the rent in the so-called “marketplace.” (That’s what happens when healthcare is treated as a commodity.)
I’m not an expert, but my introduction to the challenge came by way of two main sources: Maggie Mahar’s “Money Driven Medicine” and Paul Starr’s “Social Transformation of American Medicine.” Both point out the wide disparity and inequity of healthcare in America, and the scarcity of good outcomes at remarkably good costs. Names like Mayo, Cleveland, Kaiser and a few others kept coming up.
When the ACO concept was being crafted I was optimistic, but the end result has been way short of the dream. Toss one more trial into the error bin.
If ACO bonus payouts and setup costs are included, the reality is that they increase cost of care.
Anish, if I distill your article, it is that the people who dreamed up ACOs are pretty far removed from care delivery, and that (nod to Uncle Milty) while intent is fine, it’s results that matter. And the results are unimpressive so far. Your title speaks to “Delusion.” I’m not sure I understand that. As I see it, thus far, ACOs haven’t produced much. That’s not exactly surprising given decades of physician autonomy and volume production. It takes time and unfortunately a change in the flow of money to change that, and it won’t happen overnight.
I would ask if you agree that we must change how healthcare is delivered, and to do that, we must change how it’s paid for. I assume you’d say yes. Then to change how it’s paid for, we have to have agreed upon measures of quality of care and outcomes and pay on those bases (with risk adjustments to account for patients like Mrs. K). And we must have interoperable EHRs. With me so far?
If you agree, then something at least directionally like ACOs are needed, no? If not that, then what? Not same old.
What has troubled me is the unwillingness of most ACOs to take on meaningful downside risk. Without that there will be no change in behavior. More upside and downside risk is needed. And time.
As for patient “compliance,” corporal punishment is no longer allowed, and humiliation is tacky, so all that’s left is some other meaningful way of implementing accountability in someone like Mrs. K. I’m hardly a psychologist, and penalties are frowned on by the ADA, Title VII and GINA. My sympathies are with you. Perhaps we need to make it some form of wicked cool (I’m from Massachusetts) game show with awesome prizes that would cause behavior change.
The same physician who sees 20-30 patients a day, and deals with the ever growing cost and time of regulatory demands. The govt via ACO’s then offers $4 per pt per month to care coordinate. Yippee.
The ACO is the government’s way to have the physicians be the bad guys and ration care.