By ANISH KOKA, MD
 Safe, appropriate, effective care at a reasonable cost. Such a simple goal. The message is clear. Leaders in hospitals, congress, and even my chihuahua echo the dawning of a new age in health care. Down with the private practice, fee-for-service mentality, they all say. I pay attention to a lot of this chatter since I happen to be in private practice. I split my time on the internet between the latest exploits of the Kardashians and gravestones for my practice. I can picture the epitaph:
Safe, appropriate, effective care at a reasonable cost. Such a simple goal. The message is clear. Leaders in hospitals, congress, and even my chihuahua echo the dawning of a new age in health care. Down with the private practice, fee-for-service mentality, they all say. I pay attention to a lot of this chatter since I happen to be in private practice. I split my time on the internet between the latest exploits of the Kardashians and gravestones for my practice. I can picture the epitaph:
In loving memory of
Koka Cardiology
3/1/2013 – 3/1/2016.
Shed not for her the bitter tear
Nor give the heart to vain regret
‘Tis but mere ashes that lie here
The gem that filled it sparkles yet
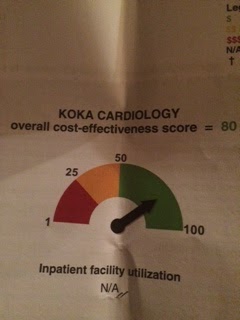
As I shuffled towards this abyss, my reverie was broken by a letter. It was from Independence Blue Cross (IBC) in Pennsylvania. It was titled: The Cardiology/Invasive Cardiology Comparative Cost report. It looked like a report card, so I opened it with some trepidation.
My first impression? I was in the green! That was good. Maybe the headstone could wait. They like me. They really, really like me. Of course, then I kept reading, and the headstone popped back into my head.
I wasn’t that good. I scored an 80 out of a total score of a 100. In the cost-effective outpatient category in the city of Philadelphia, there was a green category and a danger zone orange category. I was comfortably in the green category, but within the green category I was 21st out of 26 sites.
Great.
I started a solo practice in March of 2013. I had been out of fellowship for two and a half years and parted ways with a local cardiology group with the firm belief that I wanted to be different. I had learned a lot in my two and a half years, and lived through the mass migration of private cardiology practices to hospitals. Everyone I told about my plans to start private practice in this climate said I was crazy (and they were being polite). The private practices that were rushing to join hospitals were doing so out of desperation, primarily because of large cuts that had been made to imaging reimbursements in 2008. Alarmed at the rapid growth of imaging studies in the outpatient setting, CMS had instituted a 36% cut to myocardial perfusion imaging reimbursement, and a 25% cut to echocardiogram reimbursement in 2008. This was clearly incredibly painful to many practices that had a cost structure based on high margin imaging revenue. Practices were faced with tough choices. Luckily CMS had a reserve parachute handy – hospital outpatient prospective payment (HOPP). Physician practices leased themselves to hospitals – and voila – no more reimbursement cuts.
This was the climate I started my practice in. I did have some advantages relative to the established practices around me. Unfortunately, I was no more affable, intelligent, or more attractive than my colleagues. But most importantly, I had no fixed cost structure (technicians, underproductive physicians, or costly equipment), which gave me the freedom to set up a practice that was
not dependent on imaging. Since I was trained in the world of
CARP (limited/no role for preoperative coronary revascularization) and
COURAGE (medical management of stable angina is equivalent to revascularization), I decided to forgo an in-office stress lab. If a patient needed a stress test, I would have it done at one of the nearby hospitals. I focused on being accessible to subspecialists, surgeons, and patients. As a result, after two years of being in practice, only 7% of the revenue for the practice comes from echocardiograms or the supervision/interpretation of a stress test. I saw ~3500 outpatients in 2015. I did 537 echocardiograms, and personally supervised the ECG portion of 48 stress tests. 13% (537/3500) of my patients had an echocardiogram, which contrasts with a national average from
Medicare data of 20%. I was paid ~ $144 per echocardiogram, and $23 per stress test I supervised. In contrast, the hospital was paid ~
$400 per echocardiogram performed, and
$1140 per stress test.
In the cat and mouse game providers and payers love to play, the payers, of course, noticed that practices like mine are a fairly good deal. The medicare payment advisory commission (
MEDPAC) specifically cited the differential reimbursement of echocardiograms in recommending that this playing field be leveled. The reason for the difference in hospital reimbursement has always been explained by the significantly higher cost of doing business hospitals have relative to outpatient practices. I don’t have to comply with JCAHO and I don’t have to staff a 24/7 ER that must take all comers regardless of ability to pay. However, there is something fundamentally rotten if the patient mix, the providers, the equipment, and the physical space are the same, but the addition of the hospital logo doubles or triples the price of the service being delivered. MEDPAC has recommended in 2014, and
again in 2015, that “Congress should direct the Secretary of Health and Human Services to reduce or eliminate differences in payment rates between outpatient departments and physician offices for selected ambulatory payment classifications”. IBC took a different approach. IBC set up programs that would allow for bonus payments to doctors who practiced high value/cost effective care. In order to guide test/consult ordering physicians to cost effective facilities/providers, a comparative cost report for each facility in a certain geographic area was generated and distributed. This report was meant to highlight those providers that were practicing as hospital outpatient facilities. This was the report I had received.
Sure enough, all the ‘penalties’ (those facilities marked in orange/red) in the report were for facilities that were hospital outpatient practices. Certainly, a very interesting first step by a private insurer to use data to give physicians information about the cost of procedures. This does, though, provide yet another opportunity to look at why one has to be so careful about what quality metrics actually tell us.
I called one of the medical directors at IBC to inquire about how exactly the score was arrived at, but I only got the general information that the cost/procedure performed was the primary determinant of final score. This did serve to explain why I ranked 21/26 in the ‘green’ category. Even though I did not have a stress lab and did fairly few echo’s or stress tests, those stress tests I did do were at a local hospital at the ‘hospital rate’. I was actually encouraged by the medical director at IBC to get my own stress lab! Interestingly, a physician practice that did echocardiograms on 50% of its patients would come out smelling like a rose to the IBC folks. Meanwhile, a hospital based practice that only tested 5% of their patients would be penalized.
So much for this particular score. I understand this report as a first step that does deliver some good data, but I surmise that a lot of resources and capital went into generating a list that essentially tells you which practice is hospital-based, and which isn’t. I’m not sure how much that cost IBC. I would have done it for half (I hope someone at IBC reads this :-)).
Saurabh Jha,
Lisa Rosenbaum, and
Rocky Bilhartz are a few fellow physician who have spoken eloquently about the pitfalls of quality metrics. As I look down the list of facilities I am being compared to,
Iknow who the most efficient, highest value providers are. The challenge of quantifying this effectively in a reliable manner remains a vexing one.
Anish Koka is a cardiologist. He practices in Philadelphia.








It’s really wonderful blog & too much informative. It helps me quite a lot regarding my father cardio problem. I also read a blog post related to cardio. I hope you could read & like it & many people could get help from these type of blog post.
The original Source: https://www.trustmedi.com/blogs/running-a-perfect-cardio-heres-why