 What to do about the seemingly inexorable rise in health spending has been the central health policy challenge for two generations of health economists and policymakers. In 1965, before Medicare and Medicaid, health spending was about 5.8 percent of GDP. In 2013, it was nearly 18 percent. And GDPquadrupled during this same period.
What to do about the seemingly inexorable rise in health spending has been the central health policy challenge for two generations of health economists and policymakers. In 1965, before Medicare and Medicaid, health spending was about 5.8 percent of GDP. In 2013, it was nearly 18 percent. And GDPquadrupled during this same period.
Over the past 30 years, there are been two warring political narratives explaining health spending growth, with two different culprits and indicated remedies. At their cores, these narratives blame the main actors in the health care drama—patients and physicians—for rising costs.
The Conservative Narrative: The Patient As Culprit
The conservative thesis holds that the demand for health care is unlimited because it has been, historically, a free good for many patients. Moreover, the argument runs, much illness is driven by bad personal health choices — for example, smoking and obesity, and the heart disease and diabetes that follows. Thus, much of our cost problem is actually the patient’s fault.
Since patients have historically paid a relatively small fraction of health costs, the conservative remedy is that patients must have more “skin in the game,” that is, pay more of the cost themselves. If we do this, people will exercise more discipline in their personal health habits, and also “shop” for care when they need to use it, and costs will go down.
Adherents to this explanation point to Joseph Newhouse’s nearly forty-year-old RAND health insurance study which showed that patients who shared some of the cost used a lot less care and were, apparently, no sicker at the end of the study period. The oft-ignored coda to the Rand study was that patients were incapable to distinguishing high-value from no-value care, a finding echoed just last week by a study of patient behavior in a high-deductible health plan.
This thesis — that lifestyle and indiscriminate use of care are the main drivers of heath spending — has led to multiple remedies: health savings accounts; higher cost sharing; higher patient front-end cash payments to doctors and hospitals; and also “price transparency” — attempting to clarify in advance of care what something will cost, so patients can use their own money to shop for care.
The conservative narrative had an influential role in shaping the structure of private coverage under the Affordable Care Act, where very high deductibles and annual out-of-pocket limits are the norm, as well as the Cadillac Tax on so-called “high value” health plans, designed to discourage first dollar coverage. It has led to a quintupling of patients with high deductible plans since 2007. According to the 2015 Kaiser Family Foundation Health Benefits Survey, patient cost sharing has grown six times as fast as wages since 2010.
The Progressive Narrative: The Physician As Culprit
The “progressive” narrative is more convoluted and absolves the patient of blame. The progressives’ culprit is the way we have traditionally paid for care: fee-for-service payment of doctors and per-admission or per-procedure payment of hospitals. Progressives, and many in the health policy community, believe that cost growth is actually driven by doctors and hospitals seeking higher incomes. The piecework incentive encourages hospitals and doctors to over treat or renders care that is completely unnecessary.
Physicians, it has been argued, have target incomes; to reach those targets, they will induce demand for care, e.g. find things to do to us solely to generate income. Reform advocates argue that if we change incentives to doctors and hospitals and compel providers to emphasize prevention and more effective care (paying for “value instead of volume”), costs will fall.
The behaviorist model of physician behavior has led to so-called “value-based payment” and the Physician (PQRS). This model has also now led to MIPS, the payment incentive model embedded in the 2015 Sustainable Growth Rate physician payment fix.
The core belief seems to be that if we can find the right “operant conditioning schedule” (per behavioral psychologist BF Skinner), physicians will do higher value works at lower patient risk. The result has been a regime of “micro-accountability”: astonishing increases in clinician reporting requirements from Medicare and commercial payers, and in the amount of time caregivers spend typing information into the patient’s health record in order to get paid. It has resulted as well in vast consulting and information technology outlays by providers to support new, highly complex payment approaches like the Accountable Care Organization and the Patient Centered Medical Home.
Dissecting The Narratives
Problems with the conservative perspective: ignoring social factors. There are significant problems with both these narratives. On the conservative side, it is true that some behavioral issues, notably obesity and smoking, have major health cost consequences. As the graphic indicates, however, health behaviors account for a minority of health costs. It is laughable to think that minute or even significant economic incentives to the patient will negate the health effects of social determinants (poverty, lack of education, unemployment, compromised access to care), or of hundreds of billions spent advertising cigarettes, fast food, alcohol, and sugary snacks, or for that matter or of flawed “official” nutritional advice — let alone the accumulating effect of chronic disease as we age.
Exhibit 1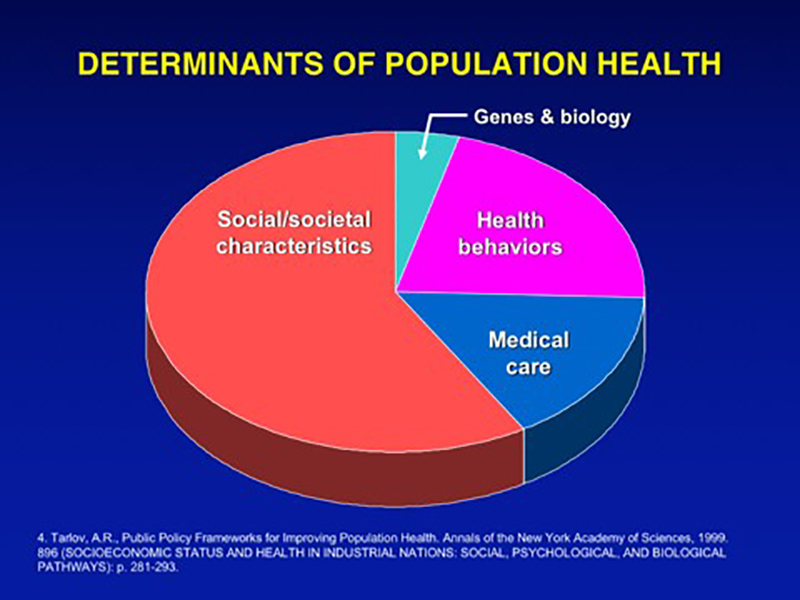
Reversing these problems is fundamentally a public health and political challenge that requires a multi-faceted approach with a lengthy, uncertain payoff. As we have seen with the sharp fall in adult smoking rates, and more recently, the accelerating decline in soft drink sales, progress is possible even if maddeningly slow to manifest itself.
The US significantly trails most OECD countries (to whose health systems ours is often unfavorably compared) in social spending. There has also been a lagging and inconsistent investment in public health in the US, despite the coverage gains from the Affordable Care Act.
To improve peoples’ health involves not only more consistent public health and social investment, but also a more just society and a more vibrant economy. In other words, improving health requires changing the society itself, not merely changing individual behaviors. There is clearly a piece of avoidable health care demand attached to changeable behaviors, but it is a lot smaller than its advocates believe.
Problems with the progressive approach: the explanatory limits of physician income maximization. On the progressive side, it is inconveniently the case that most of the countries to whom our US system is unfavorably compared (Switzerland, France, Germany, Canada) pay their hospitals and physicians on a piecework basis pretty much the same way we do, albeit with macroeconomic caps on total spending (e.g. global budgets). My spies in these countries tell me that their physicians do tend toward growing their incomes, but within definable, politically enforced limits.
But even inside the US, the “physician income maximization” hypothesis doesn’t explain why we have physician communities as diverse as Grand Rapids, Michigan, the two Portlands (Maine and Oregon), and Richmond, Virginia, where aggregate spending per capita for both Medicare and commercially insured patients is much lower than in most of the sunbelt or the northeast. Medicare’s payment methods are identical in all these places, and yet some physician communities practice a fundamentally more conservative style of medicine.
But most inconveniently of all, the income maximization hypothesis does not explain the sudden and sustained slowdown in spending we’ve experienced since 2008, with health spending growth subsiding to less than 4 percent annually. Health spending hasn’t grown this slowly in 50 years, since before Medicare and Medicaid, and spending has persisted at low levels seven years into an economic recovery.
Exhibit 2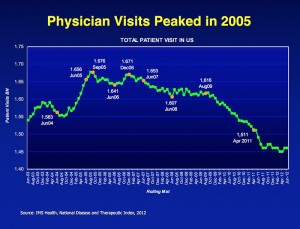

Though there has been a recent modest uptick in health spending growth, core costs (e.g. hospital and physician services) have continued growing at pre-Medicare levels through 2014 and 2015 according to recent from the Centers for Medicare and Medicaid Services (CMS). The biggest outliers in the recent cost breakout: a single expensive new drug, Sovaldi, and sharp upticks in the cost of government administrative expense and the “net cost of health insurance” — both factors linked to implementing the Affordable Care Act.
The physician income maximization hypothesis also fails to explain the loss of 200 million physician visits since 2009, according to IMS Health. Did the irresistible lure of an open cash register suddenly end in 2009? Or, are other, more powerful forces at work, such as the retirement of activist baby boomer docs or the repricing of health services to the consumer due to the growth in high deductible plans? Only time and research inquiry will enable us to understand the reasons.
Progressives not only overestimate the effect of incentives on professional behavior. They also overestimate the capacity of the health system to improve the health of the population. Health care providers have negligible leverage to influence the social determinants of health or to significantly delay the onset of age-related chronic illnesses. Even with superb primary care infrastructure, the care system is a blunt instrument in improving the public health.
Health systems spend tens of billions every year in community benefit activities, many of which are targeted at community education, screening for controllable chronic diseases like heart disease and diabetes, sponsoring wellness activities that target increasing physical activity and improved nutrition, etc. This is all to the good.
But as long as health systems’ asset base and the bulk of their professional activities are devoted to caring for the sick and injured, acute care and mitigation of patient suffering will legitimately remain their core business.
Most care givers will never care as much for patients they are not seeing as the patients in front of them. Their fundamental moral and social obligation is to those immediately at risk for death or serious systemic injuries who have nowhere else to turn than the care system. Being complaint driven, the care system is inherently reactionary, as is any safety net.
Transcending The Two Narratives
On the other hand, there are big and reachable savings to be had for society and big benefits for their patients by eliminating wasteful use of resources when people do become ill, as well as by eliminating the iatrogenic causes of illness through improved safety and protocol-driven care. Health systems are striving to make more thoughtful use of the professionals who make up their operating core, by empowering them to continuously improve the care process. Care driven by evidence-based protocols, rather than inspired professional improvisation, can only help.
In the meantime, the twin demeaning narratives of moral failure—by individual patients according to conservatives and by caregivers according to progressives—continues to animate health policy and drive us toward simplistic marginalist economics solutions that reduce physicians and patients to merely economic actors.
The real story of what creates health and drives health spending is far more complex than these cartoon narratives suggest.
We need a more complex and balanced explanation of what creates health, and a more comprehensive set of solutions that implicate public health and the human services, as well as individual citizens and the care system. The care system by itself cannot improve Americans’ health.
Jeff Goldsmith, Ph.D., is the president of Health Futures Inc. and associate professor of public health sciences at the University of Virginia, Charlottesville. This post first appeared in the Health Affairs Blog on October 28th, 2015.
Categories: Uncategorized








Thanks, Peter, for hte remarks. I enjoy your perspectie as I think we see things in a pretty common way. It strikes me that when I’ve seen comments from Canadians on their system, they do seem to trust the government much more than so many conservatives here. And the Canadian system does, in my opinion, a pretty good job of resource allocation. Of course it isn’t perfect. And there are few who come to hte US for care, but that number is actually quite tiny. I’ve read the literature on it. It’s an enormous conservative myth that Canadians are flocking here for care because they can’t in. Yes, there is rationing there. But it’s rational rationing. In the US, we have rationing by price. And class I think. Given the choice, I’d choose Canadian style anytime.
One more thing, it turns out, and you imply this, that once a country goes down the path of private interests in health care, it is virtually impossible to go down the single payer path. Too many interests will have their ox gored. What is probably more likely is that we will get to some consolidation of risk pools by “backing in”. More and more consolidation of payers and providers and Medicare will eventually insist in shifting risk because they will have to. That’s why things will get really interesting and that’s here now, but not in a big way. It still has a long way to go before per capita payments arrive.
Jeff, you may have “contributed” the equivalent of a small house (I did a quick calculaiton using tax rates and average incomes and calculate something over $100,000 in taxes over a 43-year career, assuming some average incomes rising in the later stages). That may seem like a lot (I don’t think so) until you realize that at the average per capita amount spent on beneficiaries like you of $11,200 in 2014, you and your ilk (myself included 2 years from now) will consume more than $335,000 in health care without considering any trend. That’s a really good deal. In fact, it’s too good. And why Medicare is going to have to reduce benefitss, increase taxes or reduce provider payments or all three. Medicare is already upside down and it only gets worse until Congress does something significant.
One of the key reasons I’m for single payer is that we can then allocate resources more intelligently so that we don’t spend a lot of “curative” dollars on 75 year olds (read Zeke Emanuel”s Atlantic cover of a few months back for more on why I pick that age) and spend just a few dollars on comfort and pain relief. The money ought to be spent on newborns, 20, 30 and 40 somethings so that they can perhaps avoid some of the diseases now costing us billions to treat or delay their onset, thus costing the system a lot less.
I know, I know, this won’t really happen, so there isn’t much use talking about it, but I hope you don’t complain any more about the “deal” you’re getting for the money you paid in. You will be one of the last to achieve such a return on investment. When the proverbial s..t hits the fan, all helll’s gonna break loose and those of us on Medicare then will see rates sky rocket or providers are going to get crunched. Or both. It just can’t go on.
“I’m 67 and a Medicare Advantage subscriber. I do trust that Medicare will continue to be there for me and I’ve contributed over my working lifetime enough of my income to buy a small house somewhere. I work inside the managed care framework ofmy health plan and despite a lot of health challenges in the past year, it’s worked for me.”
Jeff, if it works for you, a 67+ with challenges, why do you think it would not work for a 20 year old?
Why is contributing enough to “buy a small house” a bad thing? How big a house could you buy with your retirement savings? What would you be spending on private 65+ insurance, minus Medicare, even if you could buy it with possible pre-exist?
Good points slwrel.
Having lived under the Canadian system I have perspective on both. In Canada there is a Federal part and a Provincial part. Feds transfer money to keep the core goals of the federal mandate intact while the provinces administer the system as well as do their share of funding. Budgets, health care infrastructure and day to day policy are controlled by the provinces.
There is no free lunch as Canadians have had to continuously adapt to changing needs. The docs are private entities who negotiate their contracts with the province as well as drug companies who must operate under price controls. Hospitals are administered by boards which must stick to budget. There is no employer sponsored health coverage other than dental, which is not included in the Canadian system, and everyone has the same plan – if you need medical care, it’s covered. No co-pays or deductibles. Everyone has a provincial health ID card.
The significant difference between Canadians and Americans is Canadians are culturally committed to their government controlled and administered system, much like AARP members are committed to Medicare and SS, while Americans don’t trust government until they need government, then it’s, “send me the money”.
What does the single-pay system solve – cost control. The U.S. won’t get that until it adopts a similar system. Until then there is a patchwork of government programs as you noted trying to bandaid a system failure. Putting everyone under Medicare would be a good start.
Opponents of single-pay always say how it won’t work rather than figure out how to make it work – but as always the dysfunctional political system driven by blind ideology and money prevents fixing anything.
Canadians started early in establishing their Medicare system, before the money interests got too big to control. The U.S. now has to overcome huge financial interests which control the political system.
We got Obamacare – another corporate compromise.
I’m 67 and a Medicare Advantage subscriber. I’m living in the world I described. I do trust that Medicare will continue to be there for me and I’ve contributed over my working lifetime enough of my income to buy a small house somewhere. I work inside the managed care framework of my health plan and despite a lot of health challenges in the past year, it’s worked for me.
* I just post like a much younger person ; )
Today, there is no central management of health care. It is managed in multiple risk pools by variously skilled organizations, but only for the risk pool for which that organization is responsible. If the government “ran” the entire risk pool, yes, there would be significant problems and complaints, just as there are today. Public health could be combined with health care in general and we’d have a more coherent system. I agree that “some” of the public doesn’t trust government to manage the entire health system, and that’s why I think a public private partnership is preferable from a governance perspective. But the risk pool must be consolidated along with data.
The only way to reduce administrative cost significantly is to have everyone in the same risk pool, with the same benefit plan. Then we could manage the problems that will arise from allocating resources. Those are the problems we should be managing, not benefit plan and risk manipulation, data fog, and all the rest of the idiotic problems that arise in a multi-payer, non-centralized system. Both have huge problems. One is far too expensive and produces middling outcomes. The other will be too centralized but will produce better outcomes. The reason for that is the iatrogenesis that medicine introduces into the population. Reduce provider induced errors and at least some overuse and outcomes, along with life spans, will begin to improve.
The dirty secret of health care is more is not better. We’ve certainly proven that. Could the government really do much worse than what we have?
Jeff, think you’ll trust the government program called Medicare when you’re 65?
I worked in the Executive Office of the Governor of a large state, then as a policy advocate for a large academic health center before “retiring” from public policy and becoming a strategy consultant. Many of my friends and colleagues have worked in White Houses and Congress on health policy issues. I don’t think I’m cynical, just realistic.
Our health system has grown to the size of a large nation by itself. You need effective government to manage it sensibly. We don’t have that type of government right now. Thanks to ACA and the boomers, roughly half the country will be in government programs by 2025. My mantra:
per Hippocrates, at first, do no harm. The government ought, at a minimum, be a prudent purchaser of health care on our behalf, or delegate that job to health plans under sensible parameters.
And, per the blog, we ought to top up government investments in public health to keep us safe and help manage societal problems that lead to illness. We should not expect the private care system to do public health’s job. There is much to be done.
The general public does not trust government to manage the entire health system, and given the shoddy record we’ve seen from ACA implementation (federal website, state exchanges, the Co-ops, etc), not clear it has at the managerial capacity to do so.
Wow, I thought I was cynical, Jeff. I am not at all saying a single payer will happen. I am just saying that it is the only way to control costs and ironically improve outcomes and life span. As they say about democracy, it’s the worst form of government except for all the others. Ditto health care: single payer is the worst form of health system design except for all the others.
An interesting secular trend that likely won’t end any time soon is the simple fact that more and more of health care is funded by the government. Among Medicare, Medicaid, the new exchanges, the VA, Indian Health, Champus, Tricare and all of the govenrments in the US, plus the tax benefit for employers offering health benefits, you end up with more than 60% of the cost of care paid by the govenrment and individuals.
In many respects, employers have largely given up on cost control and are using cost sharing and increased contributions to premium to reduce or stabilize trend. This has the effect of making trend for payers look pretty good over the past few years but if you look at the costs for individuals, costs are increasing faster than wages or the economy by far. (Except in care and caid.) This, more than anything else, will bring even more government intervention, not less, as people look for relief. Then let the lobbying begin. You may be right about that, biut inevitably we’re moving toward government paid health care. Get used to it.
Bob I have been in Medicare a short time so am in the learning mode. I did not pick up supplemental coverage or Advantage as I am very healthy and could not justify the premiums, but traditional Medicare is pretty generous if your hospital stay is up to 60 days, after that it is about an additional OOP $106 per day to 90 days and double that over 90 – a nudge to get out of hospital.
Medicare does pay for medically necessary procedures and polices just testing for fun. A mis-code had them deny coverage to me for pre-op blood tests that would have cost me over $600, now corrected. I agree it needs to do much better at controlling stuff docs bill for and it needs power the negotiate drug prices – both of which are political decisions that create the weakness in Medicare because, A. AARP members vote and, B. drug companies fund campaigns and post political consulting jobs. Fraud control is another weakness, but beneficiaries can access their accounts online to view provider charges. I reviewed mine and discovered a double bill which I had corrected by the provider. Attempted fraud? Not sure. I think if Medicare offered a % of recovered fraud charges then, like whistleblowers, people would be more inclined to look and report.
The payments for near death care is largely the fault of right-wing Christians (mostly Republican) and gutless politicians, however Medicare does pay for hospice.
I repeat, those against government in health care love government in Medicare.
Thanks for your contribution, Peter.
I also daydream about Medicare for All, but here are three of my concerns:
– Medicare does do a fair job of holding down unit prices, but it is generally pretty awful at controlling utilization. (cf, McAllen Texas heart care)
– Medicare is popular because it hardly ever says No to a drug or a treatment or a very aged person near death.
The nations that do control spending say No all the time.
– Medicare also works because it has $600 billion to spend on about 50 million persons.
Every single worker and every single employer pays Medicare taxes for Part A, and every person who makes more than about $30K pays income taxes for the bulk of Part B financing. Medicare for All would require much higher taxes and they would be very visible.
“You expect single payer to work in our political culture?
Dream on.”
“Lord save us from Single Payer and the technocrats and academic geniuses that would build and run it.”
Jeff, all I can do is point the way to salvation.
Is our present health system working, “in our political culture”, is anything working, “in our political culture”?
Would those on Medicare say it’s not working and vote for dismantling?
You expect single payer to work in our political culture?
Dream on.
The bill would have to be written by the Senate Finance Committee, the kindly folk who gave us the 940 page Affordable Care Act.
By the time the lobbyists were finished with it, the Single Payer Act of 2019 would be 1600 pages long, amply larded with special carve outs, grandfather clauses, regional adjusters, Boards, Commissions, Institutes, disparity reducers, severity adjustments and special favors and other dispensations for key constituents and major donors. and would be just as expensive and unwieldy as what we have now.
Not for nothing does our Congress have a single digit approval rating!
Our federal government and the Congressional folk who frame and maintain it cannot do “simple” to save their lives. Influencing such legislation is already a multi-billion influence peddling business. Our political system is too corrupt to execute this seemingly simple solution,
Lord save us from Single Payer and the technocrats and academic geniuses that would build and run it.
slwrel, thanks for supporting what I have advocated on THCB for a long time. Its a lonely camp.
I’m not sure single-pay improves health, it does improve access if wait times are controlled. Canada had problems with wait times not keeping up with an aging population and its afflictions of bad hips, knees, and cataracts. It addressed the issue with a lot of investigation and public input. Wait times are now better and continually tracked – of course this raised costs.
Any system needs constant vigilance and adjustment.
I think the post is mostly right in its framing, as these arguments go. However, neither actually gets at the root problem–a multi-payer system of reimbursement. I fear that the argument between the two poles will continue to the detriment of actual reform of a fractured system. The raw truth is that unless limits are set by a government or quasi-government entity on health care spending, it will always be higher than it should be. A single payer approach is the only one that will limit spending and improve health. Conservatives reject this out of hand so it is mostly a non-starter. I do think, however, that if we took a somewhat different approach to setting national limits on health spending–a public-private entity–we might get some traction on limits. The root cause of health spending is a multi-payer system. Even if we paid fee-for-service, but did so universally no matter what health plan you are, it would be preferable to the completely crazy level of variation in reimbursment that attends to patients completely dependent upon what health plan they are in and what benefit plan they have. This is a recipe for disaster and is the cause of unacceptable levels of spending and ironically, poorer health.
I didn’t say that lifestyle doesn’t impact health. Look at the graphic. Health behaviors may account for 25% of a population’s health. That’s not no impact.
The point of the conservative narrative is that third party payment and an entitlement culture creates a situation of moral hazard, and encourages irresponsible personal health choices heedless of the cost. What is the point of all that cost sharing and all the tax code rearranging? It is to encourage/compel responsible personal conduct. And it’s 100% of the conservative healthcare solution for 25% of the problem. Oh. . . I forgot about selling health insurance across state lines!
If one person goes on Sovaldi at $84,000 a year, this effectively cancels all potential savings from 840 patients all dutifully cutting out one less-necessary doctor visit a year.
In other words, we should worry about income maximization by drug and equipment companies at least as much as income-chasing by doctors.
The desire of Americans to save lives at any cost — and our passivity toward related costs –is a large factor in our high spending.
Conservatives back it up (c.f. Terri Schaivo), and liberals are pretty silent about it.
(although Paul Krugman quipped that “the ACA does not actually have death panels, but it should have.”)
We don’t think of rationing basic education and subsidize higher education – why is health care different? Of course conservatives would love to ration education through vouchers.
“But most inconveniently of all, the income maximization hypothesis does not explain the sudden and sustained slowdown in spending we’ve experienced since 2008, with health spending growth subsiding to less than 4 percent annually.”
Maybe the market is working, its gotten SO expensive nobody can afford timely care – a success for conservatives.
“Moreover, the argument runs, much illness is driven by bad personal health choices”
Conservatives become quite hypocritical when solutions to personal health choices include a tax on those bad choices to pay for them.
Good piece Jeff.
“Claiming conservatives blame the patient is frankly a flat out lie that is beneath contempt ”
Then why are all conservative “solutions” focused on the patient. Chiefly high deductibles to “let the market decide”.
“the rise of 3rd party payment for most services”
The government controlled systems around the world doing it for about half the $ contradicts this view.
“Claiming conservatives blame the patient is frankly a flat out lie”
Framing is important, no doubt, and words do matter. But holding people responsible for their health and charging them a higher premium for behaving irresponsibly may be morally different from blaming people for their health, but there is no actuarial distinction.
I would say maybe there’s another narrative, moderate, if you will. The fault is the third party/government payer system.
In truth, as with any other “disaster” there are a multitude of factors which, when combined end in a bad outcome. This is true of plane crashes, medical errors, and even some natural disasters like Hurricane Katrina.
The combination of social/cultural factors contributing to poor health, some greedy doctors mixed in with good doctors who are just trying to do the right thing and make patients happy as well as healthy, patient and physician ignorance on costs, hospital charge-masters with no real definition of why those costs are what they are, a tort system which encourages over-testing, the list goes on and on.
Your last statement is appropriate Jeff. We need to find out what health is, how to encourage it without excess costs/spending, and we need to figure out how to pay for medical care and how to make it more affordable. It’s going to be a long and winding road.
Jeff- charitably assuming you are trying to be intentionally provocative…
the basis of most conservative POV on US health care: the rise of 3rd party payment for most services, excessive regulation adding to costs without value, government price fixing, crony capitalism, and an ever expanding safety net with fewer and fewer controls that punishes the middle class and one that is running rapidly out of other people’s money.
the vision for liberals for US healthcare — the US public education system, except there would be no ‘private schools’ allowed. Government monopsony for healthcare services. Unlimited financial opportunity for consultants and those with the right ‘pull’. Prison terms for accepting any payment for care not authorized was in Hillary Clinton hc plan in 1990s.
Claiming conservatives blame the patient is frankly a flat out lie that is beneath contempt — I would ask you to get any one of your liberal colleagues or yourself to come on THCB and say that lifestyle choices do not impact health, health care, and health care costs.
Conservatives fear rationing by the government. Progressives fear rationing by the market.
USA is the land of possibilities. And it has the unrestrained budget, imagination & moral imperative to chase possibilities. In healthcare this ethos costs a lot.
Nice piece Jeff.
This is a vapid generalization, I’m afraid.
Works with the pet analysis “US is the most expensive system in the world, therefore we need to save money by spending on ________________ . (Whatever thing I’m researching / developing)”
/ j
A researcher from UCSF recently told us ” Everyone in the developed world is doing about the same in health care. The only difference is that we are paying eveyone a lot more.” She was referring to docs, nurses, administrators… everyone.