Susannah Fox, the CTO of HHS was talking at the AcademyHealth Concordium 2015 conference this week. Her energetic call for innovation got me thinking:
Should the government be in the business of funding infrastructure for healthcare communication?
Comparable infrastructures
The governments on local, state and federal level have deployed comparable infrastructures and licensing in the interest of public health and safety:
1. Licensing of car tags while providing infrastructure for roads
2. Licensing of planes and pilots while providing infrastructure for air traffic control
3. Licensing post office locations while providing infrastructure for moving mail
How about: Licensing providers (NPI) while providing infrastructure for health data exchange “highway”?
The communicating health professional
What if providers could communicate in a secure “healthcare highway” or cloud system?
Dr. Specialist: “Hey @npi.1234567890 attached a consult note.”
Dr. Primary: “Thanks @npi.0987654321, sending 3 more pts your way with similar symptoms. (attached)”
Many problems associated with the current healthcare workflow could be solved by bringing all certified health professionals to a global communication platform. Patient safety and quality of care would improve:
1. A physician could easily reach a specialist
2. An ER could send discharge info directly to primary doc independent of participation in their “network”
3. A pharmacists could better identify possible drug-drug interactions and drug adherence/discontinuation
4. The urgent care clinic at the vacation resort could request background clinical information from PCP
Security and Privacy
There are significant concerns about security and privacy. But similar to cars or planes, people have come to expect that government will ensure that “drivers” have a license and the infrastructure we share meets some operational safety standards. Individual privacy is maintained and protected by laws which prohibit inspection or search of individuals (passengers) except under very specific circumstances.
This idea differs from open HIE in that this infrastructure focuses on enabling a communication highway between healthcare providers. Patient safety and quality of care are the priority and impetus. It should not be viewed as a data repository model, but a transactional model (getting information from point A to point B). The accumulation of data remains the responsibility and under the control of the federated network of the existing licensed players. This would be no different from the current model in which we entrust the storage of our medical information to licensed providers.
Enabling innovation to solve the healthcare interoperability crisis
New and innovative software solutions trying to facilitate changes in healthcare IT and interoperability are challenged by the market dominance of current vendors. Integrating novel solutions is therefore dependent on interfacing with currently deployed systems. With this healthcare information highway, new and independent innovators could plug into a network of connected providers agnostic to other vendors. This would immediately move us toward a learning healthcare system. There would also be beneficial to the current health software vendors who get instant interoperability between all their potential customers and end-users.
This infrastructure could also save millions for the public health sector. Disease surveillance and mandatory reporting would be instantly and systematically enabled and reach 100% of the licensed providers. Vital activities such as infectious disease reporting, outbreak investigations/syndromic surveillance, or registries (e.g., birth, cancer, immunizations, etc.) could all be facilitated through this infrastructure.
The geeky bits
With the federally mandated NPI we already have a logical provider identifier. The infrastructure will retain a directory with all relevant information: Identifiers, type of provider, names, geo locations, specialties, contact preferences.
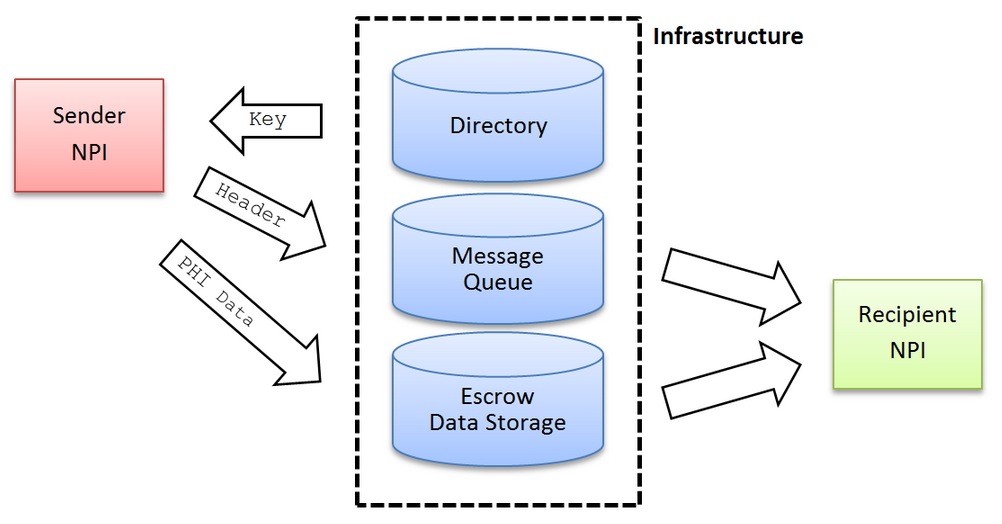
All the NPIs in the directory will be assigned a secret fingerprint. This fingerprint will only be known to the owners and the infrastructure. It would be used (like a key) to verify the communication with the infrastructure.
To initiate a message the sender first requests a communication from the directory. The directory verifies the sender using the secret fingerprint and verifies if the contact preferences of the recipient are met. If so a message key will be generated, encrypted with the sender fingerprint and transmitted to the sender. The sender then decrypts the key with its fingerprint and encrypts the PHI data (attachments) of the message with the key, then uploads the data into the escrow storage. The sender then submits the message header with the key into the messages pool.
The message pool encrypts the message key with the recipient finger print. The recipient now picks up the message header and the key. It decrypts the message key with its fingerprint and downloads the data from the escrow. The PHI can now be decrypted on the recipient side.
Is it 2020 yet?
We should learn from our past. Historically as innovation was adopted, infrastructure was enabled and built for the benefit of the public and the economy: for example trains 1830s, telegraph 1850s, telephone 1880s, federal highways 1940s, and air traffic 1950s. Initial support from government was essential to the adoption and success of these innovations. Each facilitated the transmission of information and people for the benefit of the public and our economy. Even though deregulation and antitrust acts have followed in many of these examples – initial federal investment was essential for their adoption and success.
With healthcare costs rising and the increasing need of integrated and precision medicine to enhance treatments of patients, I believe the government should take any steps needed to enable a cohesive health provider communications network. 2020: The Health Data Highway.
Adrian Meyer is Director of Systems Development at ICISS at UNC.
Categories: Uncategorized







