 Cost is the big factor. Cost is why we can’t have nice things. The overwhelmingly vast pile of money we siphon into health care in the United States every year is the underlying driver of almost every other problem with health care in the United States from lack of access to waste to fragmentation to poor quality. We can’t afford to fix the problems, cover everyone, do real outreach, build IT systems that are interoperable and transparent and doc-friendly — or so it seems, because at least on weak examination every fix seems to add even more cost. And in the old ways of doing things in health care, the way we have been used to doing business, the conclusion of the weak examination has been correct: Despite the tsunami of money, there is never enough to do it right.
Cost is the big factor. Cost is why we can’t have nice things. The overwhelmingly vast pile of money we siphon into health care in the United States every year is the underlying driver of almost every other problem with health care in the United States from lack of access to waste to fragmentation to poor quality. We can’t afford to fix the problems, cover everyone, do real outreach, build IT systems that are interoperable and transparent and doc-friendly — or so it seems, because at least on weak examination every fix seems to add even more cost. And in the old ways of doing things in health care, the way we have been used to doing business, the conclusion of the weak examination has been correct: Despite the tsunami of money, there is never enough to do it right.
Health care that costs more than it needs to is not just an annoyance; it’s a big factor in income inequality in the United States. The financial, physical and emotional burden of disease are major drivers of poverty. At the same time, the high cost of health care even after the Affordable Care Act means that many people don’t access it when they need it, and this in turn deprives large swathes of the population of their true economic potential as entrepreneurs, workers and consumers. People who are burdened by disease and mental illness don’t start businesses; don’t show up for work; and don’t spend as much money on cars, smartphones and cool apartments. Unnecessary sickness is a burden to the whole economy.
How did we get this way? What was the mechanism that differentiated U.S. health care from all other advanced countries? The usual suspects (such as “We have the most sophisticated research and teaching hospitals,” or “It’s the for-profit health insurers” or “Doctors make too much”) all fail when we compare the United States with other sophisticated national systems such as those in Germany and France. Other countries have all of these factors in varying amounts — private health insurers, world-class research, well-paid physicians — and cost a lot, but still spend a far smaller chunk of their economy on health care. Blame has been leveled in every direction, but in reality no single part of health care has been the driver. The whole system has become drastically more expensive over the last three decades.
What’s the Mechanism?
Since the difference between the United States and other countries is so large and obvious, there should be some way we can look at health care spending that would make that mechanism jump out at us. And there is a way.
The Organization for Economic Cooperation and Development (OECD) gathers and publishes huge amounts of information about the top 40 or so national economies in the world. Go online and search for its database on national health expenditures as a percentage of each country’s economy. Don’t just look for recent data. We already know what that says: The United States throws twice as large a chunk of its economy into health care as most other countries; 50 percent more than the most expensive other countries. No, take the search back to the middle of the last century. Pull the data into a spreadsheet. Make the spreadsheet into a graph. Here’s what you get:
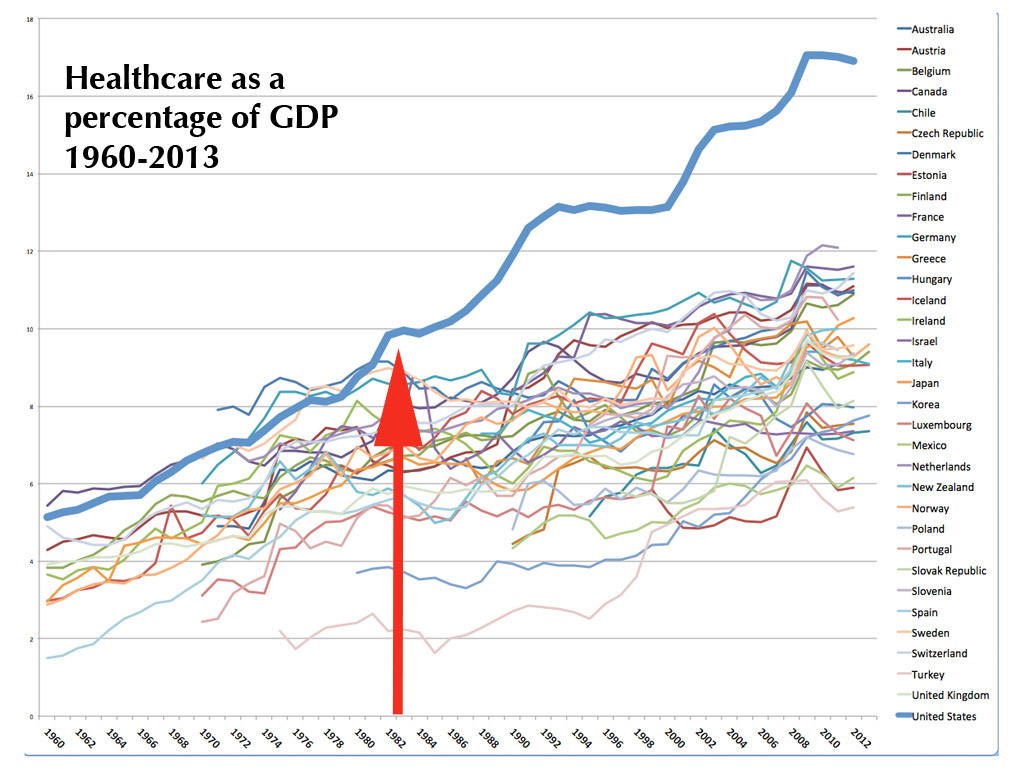
Wow. Suddenly a rather startling pattern emerges. Right side: Yes, the United States costs twice as much. Left side: Didn’t use to.
As economies grow in absolute size, they tend to dedicate a greater percentage to health care. After a certain point, somewhere around 9 percent, the cost continues to increase, but the rate of increase tends to flatten somewhat. Through the ’60s and ’70s we can see that happening. The United States, as the largest economy, is one of the most expensive, but it’s just there at the top of the pack. In the mid-1960s Medicare is implemented — the first big infusion of federal money into the health care economy — and does the U.S. line jump up? Not really. It flatlines for a year, then continues its moderate climb.
Something Wicked This Way Comes
Then something happens which is stark, sudden and large. Health care economies tend to lag national economies by a year or two; in bad economic times governments and private purchasers can’t cut health care expenditures immediately, but they do tighten their belts for the future. At a moment when the other most expensive health care economies (Germany, Sweden, Denmark) are flatlining or drifting lower in response to the global economic malaise of the early 1980s, the U.S. line goes nearly vertical, flatlines for a year or so, then leaps ever higher in a series of startling S-curves.
That first big leap is between 1982 and 1983. What was different in 1983 that was not there in 1982? DRGs, diagnosis-related groups — the first attempt by the government to control health care costs by attaching a code to each item, each type of case, each test or procedure, and assigning a price it would pay in each of the hundreds of markets across the country. The rises continue across subsequent years as versions of this code-based reimbursement system expand it from Medicare and Medicaid to private payers, from inpatient to ambulatory care, from hospitals to physician groups and clinics, to devices and supplies, eventually becoming the default system for paying for nearly all of U.S. health care: code-driven fee-for-service reimbursements.
Cost Control Drives Costs Up?
How can a cost control scheme drive costs up? In a number of ways: In an attempt to control the costs of the system, the DRG rubric controlled the costs of units, from individual items like an aspirin or an arm sling to the most comprehensive items such as an operation or procedure. The system did not pay for an entire clinical case across the continuum of care from diagnosis through rehab; or for an entire patient per year on a capitated basis, which would capture the economic advantages of prevention; or for an entire population. While it is more cost-effective (as well as better medicine) to provide a diabetes patient with medical management, in-home nursing visits and nutritional counseling rather than, say, waiting until the patient needs an amputation, the coding system actually punished that efficiency and effectiveness. Under this system, we got paid for our inefficiencies, and even for our mistakes: Do-overs would often drop far more to the bottom line than the original procedure did.
The system punished, rather than rewarded, spending more time with patients, trying to help patients before their problems became acute, or maintaining a long-term, trusted relationship with patients. Under a code-driven fee-for-service system, getting serious about prevention and population health management would be a broad road to bankruptcy.
If extra items were deemed necessary (an extra test or scan, say), there were codes for that, and reimbursements awaiting. In so doing, the system rewarded doing more (“volume”) rather than whatever would be the best, most appropriate, most efficient treatment path (“value”). It provided a written, detailed catalog of reimbursements which rewarded diagnoses of greater complexity, rewarded new techniques and technologies with new and usually higher reimbursements, and especially rewarded systems that invested in a greater capability to navigate the coding system. At the same time, the reimbursements were constantly open to pressure from the industry. Each part of the industry, each region, each specialty, each part of the device industry, became fiercely focused on keeping those reimbursements up, and getting new codes for more costly procedures.
The business and strategic side of health care became a matter of making money by farming the coding system. Do more of what gets better reimbursement, less of what does not. Make sure every item gets a code and gets charged for. The codes became a manual for success, a handbook for empire.
The Smoking Gun
The smoking gun is right there in the chart, at the big split between the trajectories of the United States and other countries. And today, at this moment, the code-based fee-for-service payment system is still by far the basis of the majority of all revenue streams across health care.
The unifying factor between multiple new strategies unfolding in health care right now, including patient-centered medical homes, pay for performance, bundled prices, reference prices, accountable care organizations, direct pay primary care and others, is to find some way around the strict code-based fee-for-service system, either by avoiding it entirely or by adding epicycles and feedback loops to it to counter its most deleterious effects.
There is no perfect way to pay for health care. All payment methods have their drawbacks and unintended consequences. But the code-based fee-for-service system got us here, and any path out of the cost mess we are in has to get us off that escalator one way or another.
Joe Flower is a healthcare futurist and contributing editor for THCB. This post was first published on the American Hospital Association’s Hospitals and Health Networks Daily May 19, 2015.
Categories: Uncategorized








“government “get out” is not a solution, simply because your risk (and mine and everyone’s) of incurring massive healthcare costs varies randomly”
That is why insurers exist. Government is not an insurance agency.
“most of us will take the easy path and not insure until it is too late. ”
What is your proof? Do you own a home? Do you insure it against fire? Why? …because you don’t want to lose a large percentage of your assets. Do people insure for healthcare voluntarily? Yes. Why? …because they want to protect their assets.
When the provider charges directly the patient, he uses his own code based system–probably very flexible. See below.
When the provider invoices an insurer he always uses–the world over–a code based system.
If the provider in the US begins invoicing or claiming in a value -based service, he will still have to use a code based system. It will only be different in that the codes signify groups of services and goods, each of which will revert back to the finely granular code of yore.
All the internal billing within ACOs, closed panel vertical HMOs, PPOs, Integrated Health Systems, etc.has to ultimately be based upon the original granular code. There is all kinds of internal billing in Kaiser using the CPT and ICD systems.
My point is that there is no way to get away from a code-based billing system unless you have a very loose direct provider to patient billing based upon idiosyncratic needs and sympathetic feelings, similar to a lemonade stand.
You are so right!!
Same with education.
Joe, I am not an expert on Kaiser, but you can find a lot of complaints on the web from people who think that Kaiser cut off their cancer treatment too early. In other words, maybe Kaiser is trying to cut down on questionable care — but there is not enough questionable care out there to make a big difference in overall costs.
I have studied Medicare claims, and what I found is that the largest costs came from care that probably worked — transplants, chemo, blockbuster drugs. Yes it worked, but at what cost?
Something is keeping Kaiser’s insurance premiums about the same as the fee for service companies. I would love to know what that something is. I do not think that surgeon’s salaries are as large a factor as you imply.
This is a very complicated issue.
To say that fee for service is the problem, however, is way too generalized.
What is needed, in my opinion, is a more personal touch from some of these “free market” firms that specialize in personal patient care, a real hands-on approach.
One firm we are looking at has, apparently, been able to reduce health care costs of the significant users by 10% a year, offsetting medical trend.
At NPLH, we focus on using the actuarials to provide short term and long term benefit accruals for self funded and fully insured employers.
It is not magic; it is math.
To learn more, go to nationalprosperity.com.
Don Levit
“ I said only that our code-driven fee-for-service piecework healthcare payment system has been the escalator of our cost structure. ”
Joe that is true and I gave a reason, “third parties are paying the bill” and I went on “That is what we see today which is not a free market.” You always seem to compare your utopia with what we have today which is not a free market rather a very significantly government controlled market and a third party payer system (employer controls the choice of insurer rather than the individual) due to our tax laws. A true free market naturally controls costs and has proven itself over and over again. A free market can be obtained even with subsidies and where those working in a free market are subject to the laws of government. Even the former communist nation of China has moved in that direction and has since become an economic powerhouse.
As far as increasing government involvement and negatively contrasting fee for service with capitation you have cluttered the blogs with such statements. Socialism wasn’t mentioned in my response though your accusation says otherwise.
It seems all too often economics is left out of the argument of healthcare and pseudo populism reigns. I don’t mean ‘cost’ which is always mentioned, but the economics of what creates prices. In this piece you focused on codes (an organized naming system), something needing to be discussed, but the codes don’t necessarily have to mean higher costs as I explain above.
I did not suggest capitation as the answer, nor did I suggest that more government control is the answer. Nor did I say anything about capitalism vs. socialism. That argument is completely orthogonal to the argument I am making. I said only that our code-driven fee-for-service piecework healthcare payment system has been the escalator of our cost structure. Any alternative payment system (and likely a fertile combination of different payment systems) will get us off that escalator.
> Other countries have a single payer system, the US does not.
Not actually true, on either end of the equation. Other major OECD countries have a wild mix of healthcare economies, from totally government owned to single payer to totally private.
And we do have a single payer system — for people over 65. It shows just how a single payer system (“Medicare For All”) would work in practice in the U.S. It is somewhat less expensive and more efficient. It is not half as expensive or massively more efficient. It pays for many of the types of waste that drive our system costs up by at least 50%, and is subject to the same kinds of gaming.
The difference is not single payer vs. not. It’s not even fee-for-service vs. not, since many of these countries (such as Canada) do pay fee-for-service for at least parts of healthcare. The difference is specifically in the way we have implemented code-driven fee-for-service piecework healthcare in our culture and political system, and allowed it to be gamed for profit.
I agree broadly, but just having the government “get out” is not a solution, simply because your risk (and mine and everyone’s) of incurring massive healthcare costs varies randomly and usually invisibly across the population. Some risks we can control somewhat, most risks we cannot, and we cannot even know them. You could have a stroke while reading this, I while writing it. It is a classic case for some kind of insurance, and the pool has to be as wide as everybody who is at risk, simply because we are all so terrible at estimating our own risk, and most of us will take the easy path and not insure until it is too late. So in a real world, with no government intervention at all, you rapidly end up in a situation where only the massively rich can pay for those huge healthcare crises in their lives without going bankrupt, and at the same time healthcare will not be able to provide the high tech services and massive organizational backup it does today, because it will be hugely underfunded. So even if you are really really rich you will not be able to buy really great healthcare at any price.
There are certainly ways of using market forces to tremendously cut the cost of healthcare, but simply having government abandon the field is not a satisfactory solution.
Thanks for putting a bit more detail on the picture, jk.
This is not really accurate. None of the other top OECD countries have perfect systems or are free from waste and chicanery. Still, there are many differences between our system and theirs (besides caring for everybody). They typically do not jump right on the bandwagon for the latest technologies. They typically have a much stronger primary care system, with fewer references to specialists where they are not really seriously needed. The have a much stronger regulatory environment for private health insurance, which cuts down a lot of the transaction costs of getting paid. They are far more likely to have really active population health management programs, reaching out to young pregnant women for pre-natal help, for instance, or managing diabetes across populations. The pay of the docs and the administrators is part of a much more pervasive pattern that adds up to seriously lower cost.
You are right that Kaiser’s costs have gone up as well. But Kaiser works within the same healthcare economy so, for instance, they hire a back surgeon in a market where waste has driven the value of back surgeons up enormously. And their general ability to extractor premiums from users and the government is in the context of a wasteful code-driven system. They get their economies and cut waste in some ways, but are not forced strongly to abandon all wasteful practices. If they, for instance, just cut out all back fusion surgeries for simple back pain and such, they would lose market share to other providers who will offer it. That will only change when more of our providers are paid differently and no longer find it profitable to offer useless or harmful and wasteful treatments.
“Because the people who work in health care get higher incomes, and they buy a hell of a lot of new cars and start a lot of new businesses. Just in crude observations, check out the new cars in a hospital employee parking lot”
__
That may well change, sooner than we think.
http://tinyurl.com/lyjqpsm
I would like to offer two observations regarding Joe’s excellent and thoughtful article.
1. I believe that Kaiser Permanente’s costs have gone up also, and they are a devoted opponent of fee for service. Kaiser’s retired chief George Halvorson is someone I have followed for 20 years (we were both Minnesotans), and George’s writing focuses on new technology as a cost driver just as much as milking the fee schedules.
2. Joe’s paragraph about health care costs hurting the economy is just incorrect in my view. He states that sick people buy fewer cars and start fewer businesses due to high health care costs….and this is true but it is not the whole story.
Because the people who work in health care get higher incomes, and they buy a hell of a lot of new cars and start a lot of new businesses.
Just in crude observations, check out the new cars in a hospital employee parking lot,
And in my personal life– I have been harmed by medical debt and high insurance premiums, but I make a living at health insurance also.
Smoking is the biggest cause of cancer…Leave smoking now before you die…world tobacco day is coming on 31 may….Save someones life…read more about it on
http://www.thetechsea.com/2015/05/what-is-world-no-tobacco-day-how-to.html
http://www.thetechsea.com/2015/05/best-world-no-tobacco-day-2015-quotes.html
You would think that all the money pouring into health care would make quality better. But we are seeing certain abridgements simply owing to high prices. Docs are hesitant in ordering genomic cancer markers (e.g. androgen receptors in triple negative breast tumors) and they restrain searches for all-but-banal co-morbitities, e.g. hemoglobinopathies and porphyrias.
Price regulation by the government via Medicare is tough to single out as the principle root cause of higher costs for US health care. The factors vary by category.
For hospitals, it is the institutionalization of historical cost as a basis of reimbursement for hospitals, reflected in DRG’s customized to individual hospitals rather than established on a local or regional reference pricing basis, that has taken competition out of the equation. Countries which use a fixed budget or capitated population-based reimbursement model tend to do a much better job at controlling hospital costs.
For physicians, it is the resource based relative value scale reimbursement model which has fueled massive increases in specialty incomes while providing disincentives for primary and preventive care. Reimbursement models which emphasize efficiency and quality of care, while providing safe harbors against malpractice which fuel defensive medicine and overtreatment, make sense here.
And as for prescription drugs, the need to replace a high risk-high reward FDA approval and patent licensing process with one which continues to reward true medical breakthroughs while enhancing cost-effective access to medications is sorely needed as well.
There are opportunities galore here for improvement.
Great Post..
Source: http://www.tariqdrabu.co.uk/
Good Allan. Bingo.
There is an MD speaker at UCSF grand rounds who tells us that all the OECD countries are doing almost exactly the same in health care. The only two differences she says is that the US pays its docs a lot more and its administrations much much more. I wish I could recall her name. Someone on this Blog–during a previous exchange– did know her.
Not only did DRGs start in 1983, but also that same year CMS adopted the AMA’s CPT codes as its payment mechanism for Part B in 1983. The combination of the two was, in effect, a massive regulation of the industry. And regulation always raises costs. But dtaylor379 is also correct: it was the presence of a willing payor that allowed providers to turn a cost-control mechanism into a revenue producing mechanism. MIT economist Amy Finkelstein attributed about 40 percent of the rise in per capita health spending from 1950 to 1990 to the introduction of Medicare: http://www.nber.org/digest/apr06/w11609.html. She found that there was a 23 percent increase just between 1965 and 1970. It may not pop out as much in Joe Flower’s graph because many of the other OECD countries started state-run health plans in the 1960s and 1970s. My city of Indianapolis was particularly fertile ground for the effects of a willing payor+code-based, fee-for-service reimbursement to play out because many of the mechanisms that offered some restraint elsewhere weren’t present here: CON laws were lifted in the mid-1980s; HMOs never gained ground here because the broad-choice, rich benefits plans of the UAW set the standard in the employer market; the health status of Hoosiers required a high volume of procedures anyway; the lack of geographical restrictions made it cheap to find another cornfield to build another hospital. As a result, when it was clear cardiovascular care was needed and would be reimbursed well, the local hospitals not only did more CV procedures, they each built their own hospital focused specifically on that. The same basic story played out in orthopedics and cancer, as well as in the most affluent suburban areas. Now all the local hospital systems have inpatient occupancies below 60% at their numerous facilities and are desperately trying to find ways to cut back on their very large fixed costs. The growth of Medicare Advantage plans plus the high popularity in Indiana of high-deductible health plans–both of which unwind some of the willing payor+code-based FFS reimbursement–are forcing some rollback on the trend Joe Flower so vividly identified. Thanks for a great post.
I submit that it is government that is responsible for the high cost of health care. We have created a “willing payor” environment which has lead to inflated charges for reimbursed procedures. The government may be good at negotiating discounts, but healthcare companies are better at coming up with high cost solutions. As well, government plays on the need for society to cover drugs and procedures that have marginal efficacy and no ROI. If you evaluate market based healthcare – lasik, cosmetic procedures… You will see products and services that have become more affordable time. This is primary because consumers pay for these procedures and providers have to compete. The government creates a “false market” that has created a system that is gamed by providers, manufactures, insurers… I submit that healthcare will cost half if government will get out!
See “In Memoriam FFS” http://onhealthtech.blogspot.com/2015/05/in-memoriam-ffs.html
I don’t doubt your analysis Joe, but there is another explanation too. Other countries have a single payer system, the US does not. This has two massive impacts:
1. The cost of administration is much higher, 25% ( http://www.commonwealthfund.org/publications/in-the-literature/2014/sep/hospital-administrative-costs).
2. The company that insures me when I am say 25 years old, doesn’t care if I’m healthy when I’m 50. They don’t care because most likely I will be on a different insurance plan by then and hence someone elses problem. The multiple payer system does not have any inherent incentives for preventative healthcare. In a single payer system, spend on preventative care is proportionally higher because the payback is greater when people get older.
“Under a code-driven fee-for-service system, getting serious about prevention and population health management would be a broad road to bankruptcy.”
That is only true when third parties are paying the bill. That is what we see today which is not a free market. Fee for service whether that payment be direct or via an insurance mechanism controls costs in a free market system. In fact the free market system has proven itself over and over again. The capitation/ government type systems you seem to suggest have failed in many ways. If you prefer capitation over fee for service why not permit the people to decide without governmental favoritism.
“ But the code-based fee-for-service system got us here, and any path out of the cost mess we are in has to get us off that escalator one way or another.”
No, government intervention based upon plans created by academics and ‘experts’ got us here. Capitalism and the free market system made us the most powerful nation in the world.