 The new “fiscal cliff” legislation hailed by some as a “one-year doc fix” of the scheduled 26.5% sustainable growth rate (SGR) cut that was scheduled to take effect on 1 January 2013, has passed the Senate and House as part of the American Taxpayer Relief Act ( HR 8 ) goes to President Obama for his likely signature.
The new “fiscal cliff” legislation hailed by some as a “one-year doc fix” of the scheduled 26.5% sustainable growth rate (SGR) cut that was scheduled to take effect on 1 January 2013, has passed the Senate and House as part of the American Taxpayer Relief Act ( HR 8 ) goes to President Obama for his likely signature.
But was this “one-year doc fix” really a fix?
Not at all.
In fact, once again Congress has failed to resolve the ever-present sustainable growth rate cuts that repetitively surface year after year by kicking the proverbial can down the road another year.
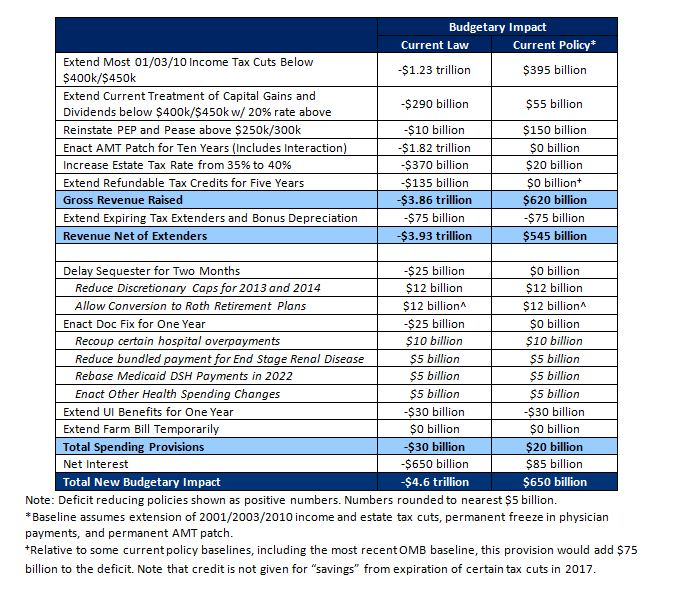
The cost of the one year patch will be $25.1 billion dollars over 10 years and will be paid for almost entirely by health care cuts in other areas.
- Hospitals (increasingly doctor-employers now, remember?) will see audits of their billings increase as efforts to recoup some $10.5 billion of “overcoding” charges are seen as the largest source of revenue for the one-year “fix.”
- Hospitals will also see an extension of lower Medicaid payments to hospitals that treat a high number of uninsured or low-income beneficiaries, known as “disproportionate share hospitals” to find savings of about $4.2 billion.
- Another $4.9 billion offset will be applied to the lowered bundled payments given for patients with end-stage renal disease – some of the sickest people receiving services from Medicare.
- Also another $1.8 billion will be “saved” to offset the “fix” by reducing payments for multiple procedures that are performed on the same day with patients. Look for more ICD-9 (or ICD-10) code changes for the new year.
- Also, look for an even greater crackdown on imaging studies as another $800 million has to be found to pay for the “fix.”
- And there’s more: the complete list of payments for the “fix,” drawn almost exclusively from health care alone, can be found here.
- Finally, doctors can expect revenue to stay flat result of this “fix” from Medicare, meaning that the payments received will not address costs imposed by annual inflation. (You well-paid primary care doctors, are you listening?)
So you see, the “doc fix” is in for another year alright …
… one that is assured to get even harder to really fix next year.
Westby G. Fisher, MD, (aka Dr. Wes) is a board certified internist, cardiologist and cardiac electrophysiologist practicing at NorthShore University HealthSystem in Evanston, IL. He is also a Clinical Associate Professor of Medicine at the University of Chicago’s Pritzker School of Medicine. He blogs at Dr.Wes, where this post originally appeared.
Categories: Uncategorized








{kind=link}
Peter, you have a point there.
All I was getting it is that if Medicare adopts a sensible policy on deductibles, then seniors with no money will put off going to the doctor.
(the way they all used to before 1965)
Rather than cobble together Medicare and Medicaid, we could just give the poorest seniors a voucher for the deductible. Rather like medical food stamps.
“Poor seniors would need a clearer access to Medicaid.”
Which pays less than Medicare. Why do you want to continue with a fractured health care system? Why would poor seniors deserve less treatment than the rest? There is only one set of providers to access.
Let me drag in my old point once again.
Why does Medicare pay for any office visits at all?
That would clear up the entire doc fix and would clear up one big part of upcoding.
Raise the Medicare deductible to $500, like tonight.
Poor seniors would need a clearer access to Medicaid.
That is not an impossible task.
If some middle income seniors are still left out, give them a $1000 debit card.
20 million seniors with a $1000 debit card is just $20 billion a year.
That equals ONE MONTH of current part B spending.
bob hertz
Point taken, rbaer. Just wanted to say that the coding game is complicated and it is much easier to bill for two or three simple visits than one complex. I am starting to see 10 minutes time slots for regular visits. A couple of years ago 15 minutes was the most common minimum for an f/u. It’s just getting worse….
Barry,
Kaiser is also a payer. Productivity is not helpful to payers. I don’t know enough about Mayo to comment. I don’t have a problem with salaries per se, but more with the nature of the employer….
As to hospitals, these PCPs they are buying are bought precisely to lock-in referrals. They are not money losers. They are loss leaders by design. It’s all about maximizing revenue. and that “collegial team oriented environment” is largely fantasy. People can be collegial nowadays without being employed by a semi-monopolistic entity.
This is pretty long, so you may not have the patience to read it all, but I am furious at the public deception campaign, and frankly a bit disappointed with all the docs… http://onhealthtech.blogspot.com/2013/01/the-crosshairs-of-triple-aim.html
Margalit –
More and more doctors are being paid on a salaried basis which I think is a good thing, at least in theory. Unfortunately, too many salaried docs employed by hospitals or large physician practices get bonus compensation tied to relative value units billed as a way to ensure some reasonable level of “productivity.” Kaiser and Mayo, to their credit, don’t compensate this way. However, there are probably a lot of doctors who can’t or won’t function very well in a collegial team oriented environment.
Too many hospitals today see PCP doctors on their payroll as money losers for the system. To mitigate those losses, they are expected to refer their patients within the system in order to drive revenue for the mother ship even if that system is not the most cost-effective high quality provider in the area. This is another reason why I’m a big supporter of robust price and quality transparency tools for both patients and referring doctors.
Maragalit,
There are a lot of great PCPs handling complex patients and re. the statement you find objectionable, I wrote “many” and not even “most” or “all”. Re. the reimbursement issue: you are right (I see a lot of poor referrals that are done in the context of 10 min ecounters), but I wonder whether these PCPs would have the option to increase coding based on complexity and/or time.
Another thing that we should consider doing would be a simple summary of benefits letter that explains what a provider did in one encounter, how much it costs and how much time it should take. With a 1-800 number for patients to call and report irregularities, and susbsequent investigations if multiple patients state that a high complexity/high risk visit with Dr. X which should last 30 minutes or more is over in 5 minutes.
Yes, taxes should go up significantly, but so should wages assuming employers don’t unanimously decide to “soak” the workers…..
And if we can reduce costs by creating a unified payment system, than most people should be better off than what they are today, and have peace of mind on top of it.
rbaer, I know quite a few PCPs who would take issue with your assessment of their abilities and their actual practice.
Unfortunately, I also know PCPs that do refer out quite a bit. The reason for that is not usually inability to treat patients, but the simple fact that payments are not really reflective of complexity and time required to treat these conditions. Changing the payment model should address this problem.
Barry, the present system shields the populace from the reality of cost/benefit. Tax free employer subsidized coverage or debt subsidized Medicare. Paying the true amount would put pressure on heath care to control costs.
That’s one reason we can’t make ant headway on cost control, Americans are living in a fairy tale.
I like Barry’s summary but I think one could save a lot of money and harm by taking away detrimental financial incentives created by the reimbursement system. Pay surgery only a little better than seeing office or hospital consults and all these useless tonsillectomies, hysterectomies, stents and back surgeries will greatly decrease.
Educate the population that more care is not always better – often useless and not infrequently harmful. If physicians would – as a rule, many but not most do – practice rational medicine (and yes, the litigational threat is real)and had a more representative association than the AMA, we would have a gigantic “more is not better” campaign, probably with the support of the White House (for instance, Pres. Obama publically refusing PSA testing in his wife’s vegetable garden).
Yes, PCPs could do (and make) more, but that would require:
-limiting the litigational threat (caps are NOT a solution)
-enhancing their education (for instance, make them really comfortable in managing moderately complex diabetes, heart disease, headache, back pain) by truly rotating with specialties during residency
-most importantly, a cultural/expectation shift. A lot of patients think the only thing the PCP can do is prescribing ABx for a cold (which BTW of course they should not) but will have to refer to specialists for most other things … and unfortunately, many PCPs accept that role.
Peter1 –
As we’ve discussed before, I wonder if most people have any idea how much in taxes they would have to pay to support a single payer health insurance system. My best guess is at least 15% of income for most middle class and upper middle class people and it could easily be closer to 20% even with current Medicare level dictated prices.
Lots of people with good employer coverage are already paying that implicitly but don’t know it. They perceive their health insurance coverage, beyond their own relatively modest contribution, as largely “free.” Maybe they think all we have to do is soak the rich some more and everyone else can have a free ride. Good luck with that.
“And every 2 to 4 years we can argue about the budget and then vote. Not old against young, or poor against rich or vice versa, but all of us in the same boat”
That’s a single pay system for all supported by taxes using community owned hospitals. Anything else pits constituencies against each other and divides income groups.
If you need to use the same facility as everyone else then you’ll want to have some ownership in how it’s run.
Bob –
The most recent data I remember seeing about the VA is that it serves roughly 5 million veterans. Since its capacity is limited, the VA divides veterans into eight different groups for the purpose of determining eligibility for VA care. Group 1 (highest priority) are those with service connected disabilities usually as a result of combat. At the other extreme, Group 8, are those with no service connected medical issues and with income above a middle class threshold. Due to this ranking system, there are many veterans that are denied access to the VA system due to capacity constraints.
You are right that hospitals are a very high fixed cost business. About 60% of revenue goes for wages and benefits. Another large piece is for utilities, insurance, property maintenance, etc. Only about 15% of revenue is spent for medical supplies that vary pretty directly with patient volume. The marginal cost to treat the last few patients when there is extra capacity is indeed quite low. There are numerous rural hospitals that operate at high cost primarily because their occupancy rate is persistently low even when they are the only hospital for many miles around. I would also note that both doctors and hospitals need some spare capacity to handle emergencies and unforeseen circumstances.
Margalit –
That’s a good summary of your concept of an ideal healthcare system. I think it would be hard to execute, though, without rationing especially if patients don’t have to pay anything, aside from taxes, for service as is the case in the UK.
I’ll also add that I love doctors. I’m alive today because of their skill and dedication and the miracles of modern medicine including prescription drugs. That said they are human beings. They sometimes make mistakes. Even they need some oversight. I also think that hospitals need ethics committees to handle the tough and close calls which are not rare.
Finally, regarding PCP compensation, my understanding is that primary care docs in the UK make as much and sometimes even more than specialists. I could see raising their compensation here to the $300-$400K range depending on the regional cost of living. That would be a sizeable bump above current compensation for most of them and I think it would be adequate.
Barry has some great points, especially when he admits that there is no silver bullet. Cost control is a long-term, grinding process, and this is true in every advanced country including Canada and Sweden and Denmark and any others that are supposed to be more efficient than the USA.
To Legacyflyer — my point about the VA hospital is that their nurses and doctors are already on the government payroll, and their hospitals do not have mortgages and bonds that need to be serviced with large payments.
Therefore, if the VA hospital has an empty bed — and some of them do have empty beds — why not put a long-term medicare patient in that bed?
I grant you, I have never run a hospital. But I think that over 80% of a hospital’s costs are fixed. The only flaw in my scheme is if the Medicare patient needs very expensive drugs.
My belief is that hospitals incur costs early on, and then they recover costs by billing patients. I am very skeptical that an additional patient really costs as much as one would think from hospital billings.
I may be wrong about this, please do not hesitate to correct me if I am.
Great summary Barry and lots of good ideas. I don’t know what the left wants, particularly if that left is represented by the current administration, which in my opinion, is erring on several counts.
I don’t want to “squeeze provider payments”. I don’t want to have “providers” at all. And I don’t want to have “ethics committees” or regulations imposed on the actual practice of medicine.
I want the medical profession to stand up and take charge of medicine, one doctor at a time. I want to have doctors, not providers of I don’t know what.
In the Hopkins case, doctors should have firmly said that the man is dead and everything we’re doing now is torture and we are not going to continue harming this patient just because you are asking us to, in very simple words without a need for diplomacy. The fact that doctors cannot do this any longer because of whatever reasons is the biggest problem we have.
I would like to create a situation where people have doctors they can trust and listen to when disaster strikes, and I would like those doctors to feel free to act in the best interest of the patient (not the family and not the government). Therefore I would like to triple or quadruple the pay for primary care physicians to match the responsibility and to allow them the necessary time to practice medicine as it was intended to be practiced.
I would leave life and death and everything in between to the individual and his or her trusted advisors. Some will choose foolishly, most will not. I don’t want us to become a nation “accepting of death”, whatever that means, and I don’t think people of other nations are either…..
I would also like to take out all the “small” profit margins of all the quick buck chasing entities who think pain and suffering and fear can be monetized in grand ways, because small margins add up to huge deficits. All businesses in health care should be social businesses in the strict meaning of that word..
The government should collect taxes and divvy them up to administrative bodies to manage the financial payments to doctors and hospitals, and hospitals should be broken into the smallest pieces that can function independently, and none should “own” office based clinics, because there are no economies of scale in health care and because prices will be set anyway.
And every 2 to 4 years we can argue about the budget and then vote. Not old against young, or poor against rich or vice versa, but all of us in the same boat (excluding the mega rich as usual).
So I don’t know if this is left or right or plain crazy, but this is what I want.
It seems to me that the debate between the left and the right around healthcare cost containment can be summarized as follows:
The left wants to continue to squeeze provider payments further. Some want a single payer system or one size fits all Medicare for everyone. Impose global budgets to force providers to become more efficient. More conservative folks like me want to change both the provider culture and the culture of often unreasonable patient expectations to reduce wasteful spending on unnecessary or inappropriate care.
Neither Medicare nor Medicaid has a successful track record in controlling healthcare costs or utilization. Both programs are riddled with fraud though the financial impact is impossible to quantify with any precision. Even if we had Medicare for all and global budgets, what would happen when the budget was exceeded by November? Given the political power of the senior lobby, I suspect that Congress would just pass a supplemental appropriation like it does for the DOD when it needs more money to fight wars. We can’t keep telling people that they can have whatever care they want when they want it, someone else will pay for it and, somehow, dictated prices and global budgets will control costs. They won’t unless we are prepared to ration care or find other ways to sometimes say NO.
My preferred approach also requires taking on powerful constituencies starting with trial lawyers, a key constituency for Democrats. At a minimum, we need safe harbor protection from failure to diagnose lawsuits for doctors who follow evidence based guidelines where they exist. Defensive medicine is also impossible to quantify with any precision but it pervades the medical culture.
We also need to proactively encourage elderly patients to execute a living will, advance directive or POLST and charge them a penalty of $10 per month on their Medicare Part B premium if they don’t. While more such documents would not eliminate expensive and futile end of life care, they could reduce it considerably.
Price and quality transparency tools for both patients and referring doctors would also be helpful to make both patients and providers more cost conscious even when insurers are paying all or most of the bill. People who get health insurance through their employer should also be informed about just how much the employer is spending for health insurance for the employee and family, if any. Patients should want to get their care from the most cost-effective high quality provider.
We should refuse to pay for new drugs and devices that are no better than competitive products but much more expensive or we should pay only the cost of the less expensive alternative and let the patient and family pay the balance if they really want the more expensive therapy. This idea is called reference pricing.
We could encourage medical tourism within the U.S. if high quality care can be obtained for significantly less money, including the cost of transportation and lodging for the patient and a companion, in a distant city. This could be a reasonable alternative for high cost procedures like a hip or knee replacement or even heart surgery.
Finally, when conservative practice patterns in certain areas achieve favorable outcomes at comparatively low cost, they need to be publicized widely. Let doctors in regions where the perceived regional standard of care is to overtreat explain why they are spending so much money with nothing to show for it in terms of superior patient outcomes.
There is no single silver bullet here but lots of silver pebbles. We’ve got a lot of work to do and the sooner we get at it, the better.
“When a patient on Medicare is going to be in an ICU for a long time, why not transfer them to a VA hospital — which is in fact already paid for in existing federal budgets?”
Oh and it won’t cost anything to take care of all these extra patients ???????
i like this topic.
When a patient on Medicare is going to be in an ICU for a long time, why not transfer them to a VA hospital — which is in fact already paid for in existing federal budgets?
There will be the usual squabbles about how to charge this off, and some patients cannot be transported, but in many cases this would work.
Again this would not be popular, because the nearest large VA hospital might be 300 miles away from the patient’s immediate family.
Someone made the perceptive comment a few posts ago that I had better not be planning to run for office on a platform of harsh cost controls in Medicare.
That perfectly illustrates what political scientists call “The fiscal illusion” in American politics. The American people have been spoon-fed the illusion that Medicare can give cadillac care to 50 million seniors (and soon to be 70 million) for 2.90% of payroll and about 4% of income taxes.
Moreover the American people think that Medicare is already paid for, through the trust fund fiction…..
Therefore voters would reject anyone like me who would say,
“you can have Cadillac care for another 5% in taxes, or you can leave taxes flat but reduce Medicare to 1970’s level treatments.”
Honesty does not pay when the fiscal illusions are in place.
“Why didn’t the John Hopkins docs put an end to the madness? Surely nobody can force them to harm a patient?”
Margalit –
Hopkins was afraid that they would be sued if they didn’t accede to the family’s wishes. Doctors tried as diplomatically as possible to explain to the family that the patient had a zero chance to recover and resume anything resembling a normal life. At one point, the family specifically suggested that they thought Hopkins wanted to stop treatment to save money while the doctors insisted that cost was not a factor in their treatment recommendation.
I’ve suggested before that we should change the default protocol in these situations from “do everything” to apply common sense depending on circumstances without doctors having to worry about being sued. Perhaps the hospital’s ethics committee should have the power to overrule the family if necessary in order to stop futile care that is putting the patient through incredible suffering to boot. Often family members can’t let go because they haven’t come to grips with their own mortality and they don’t have a clue as to what the patient would have wanted in the absence of a living will or advance directive. Many times even if there are documents that call for no heroics, their bias is to find a way to ignore or overrule them in order to continue treatment the cost of which taxpayers or insurers have to pay for.
This doesn’t happen nearly as much if at all in other developed countries because people are culturally more accepting of death when the time comes. Moreover, part of the implicit social contract in those countries is that you don’t impose unreasonable expectations and their associated costs upon your fellow citizens.
I agree with everything you wrote, although the magnitude and horror of each occurrence may be deceiving… I don’t really know…..
Patients should decide if they can, and if the family acts insanely and decides to torture the old man, the primary care doctor with whom he should have had a long term relationship should be the next best thing, but people are less likely to have a trusted doctor nowadays and the way things are advancing, people are actively discouraged from trusting doctors. So we’re left with accountants to decide…. I don’t like it….
Why didn’t the John Hopkins docs put an end to the madness? Surely nobody can force them to harm a patient?
Margalit,
“This luxury” doesn’t cost a little money, it cost a LOT of money.
And I would not even squabble if I thought that the PATIENT wanted all this stuff done. But in many cases, the patient has no voice and what is being done is being done to assuage the guilt of family members who have no real idea of what the patient is going through and what the real chance of success is.
There was an excellent article approx 6 months age, in the Wall St. Journal about the last months of an extraordinarily expensive Medicare patient at Johns Hopkins. The striking thing to me was how much pain the patient was put through by his family in a futile attempt to “save his life”.
Nobody benefited, except perhaps (in the most cynical view) Johns Hopkins – who got the revenue – but I don’t think that was their motive. Medicare spent over $1M to keep a patient in the ICU – who ended up dying anyway. According to the article, the patient was in agony much of the time. And the family, ignorant as they were, ending up having to watch this whole ugly spectacle.
What would $1M yield if spent on primary care, or pre-natal care, or vaccinations, etc. Or what would it yield if we spent it on college educations, green energy or re-building bridges over the Mississippi (that fell down).
We need to re-arrange our priorities, realize that life ends and spend our resources on more productive things that keeping ill, elderly people alive for a few more months.
Barry,
I agree with legacyflyer regarding the living wills. It’s one thing to theoretically decide and another thing to decide in the moment. I for one have no desire to tell people how they should die, or how they should live for that matter. And if this luxury costs a little money, so be it. There must be some less ethically troubled places to save money, so why attempt to walk through the thickest part of the wall?
If Dr. Emanuel who is not shy about rationing does not perceive this as a major problem, I am certainly not going to debate him on this. The entire “last year of life” is in many cases a flawed metric, unless you have divine foresight, which is my entire issue with the Dartmouth data.
As to Medicare, if we could pool the entire country in one system, the sheer notion of risk will become irrelevant, and if all those healthy young people who are now required to contribute to private enterprise, plus subsidies courtesy of taxpayers, would contribute to actually support the elders, perhaps we can finally have budgets to work with, and a huge stick to carry along….
Barry,
I agree with your idea about the penalty for not having a living will. But, please understand that when “the poop hits the fan”, some of these living wills get changed or not followed. Still, having had the discussion and thought about it in advance is good. I would also suggest that some seniors who think “everything should be done” spend a little time in the ICU and watch how many people are “saved” and what they go through.
I do think that there is a fair amount of money to be saved on drugs. I never understood why the Government doesn’t buy generic. It would save a ton of money. The only thing that I can think is that Bush got bought off by the drug companies when he came up with Medicare D. Think of the clout the Government would have if it combined the VA, Medicare and the Military in one buying consortium.
There is definitely whack-a-mole going on in Maryland.
Some of the above posters have suggested that although Maryland is a low reimbursement state, “we make it up in volume”.
While I am not knowledgeable about all procedure volumes, I can tell you that I am familiar with studies comparing volume of high tech imaging in Maryland vs. other states. Usage in Maryland is significantly lower than a number of other States (like Texas and Florida) when it comes to CT and MRI.
Similarly, Maryland has been on the forefront of restricting docs from self-referring high tech imaging studies to their own offices.
Margalit –
There are plenty of healthy seniors. In any given year, the least expensive 50% of Medicare beneficiaries (24 million people) account for only 4% of the program’s costs. At the same time, according to health policy expert Ezekiel Emanuel, the roughly 6% of beneficiaries who die each year account for 27%-30% of costs, a ratio that’s held pretty constant for many years now.
I think we would be better served to aggressively drive up the percentage of seniors who execute a living will, advance directive or POLST and store the information on a registry so it’s available to doctors and hospitals when needed. Seniors who don’t execute one of these documents should pay an extra $10 per month in Part B premiums.
We also need to change the culture of overtreatment which is driven, in large part, by patient and family expectations. The attitude of I want what I want when I want it and I expect someone else to pay for it has to change and soon.
Finally, we need tort reform that at least protects doctors from failure to diagnose lawsuits if they follow evidence based guidelines where they exist. Damage caps are not the answer. Limited safe harbor protection from lawsuits could reduce the need for defensive medicine which currently pervades the U.S. medical culture.
While there could be some opportunity to cut prices for drugs and devices through the use of drug formularies and standardizing on a limited number of devices in operating rooms, I don’t think slashing provider reimbursement rates across the board will have the desired effect you think it will.
With respect to legacyflyer’s point about care that the patient needs as opposed to wants, in the UK, they claim that every patient who needs dialysis get it. In the U.S., every patient with renal failure is offered it no matter how old and sick they are or how many other co-morbidities they have. There is a big difference between the two approaches. U.S. patients are probably unwilling to accept the UK approach as far as I can tell. Maybe some of the docs could speak to that issue.
The problem in Maryland is the whack-a-mole effect. If you’re going to control prices, you have to control all of them. This has not been truly tried.
Medicare is not a good example either, because it really is not enjoying the advantages of a single payer and price setter. First, its pool is terribly skewed to high needs people with no support from healthy ones. Second, it has political handcuffs on when it comes to negotiating prices with suppliers and even when it sets prices for services. Do you think the insurance lobby will allow Congress to approve drastic cuts to Medicare payments that will trigger higher prices for private payers? It’s the whack-a-mole again… We can’t just half do it and half don’t… It’s either or.
The record on Medicare cost control is unimpressive because nobody is willing to take a stand. 85 Y.O. demented patient with diabetes and cancer – she DESERVES the right to be in the ICU. 70 Y.O. with cirhosis, COPD, etc. – he DESERVES the right to a liver transplant. 50 Y.O. with headache – he/she DESERVES the right to come to the ER and get a CT at 11p.
What we should be signing as our National Health Care song is:
“You can’t always get what you want….
But if you try some time, you just might find
You get what you need.”
Until we start signing that song in unison, we are still re-arranging the deck chairs on the Titanic. (I do like that analogy)
Peter1,
So you agree with me that Maryland is a high cost state and has remained so for the past 30 years despite the HSCRC?
Not surprised you don’t like tort reform – if memory serves you are a lawyer right?
Nope!
As you probably have guessed from reading my posts, I would not be electable – either as a Democrat or Republican.
I expect that we will continue to go down the same path we are going – wasting Billions on tests and treatments that provide no significant benefit.
Bob –
I think it would be relatively easy to control healthcare costs if we were willing and able to ration care, especially hospital based care. I’m reminded of the oft cited comment: we can have our healthcare good, fast or cheap. Pick any two.
As legacyflyer noted, it’s just not likely that anyone in Congress is going to take on the senior lobby with respect to limiting Medicare in any way. The only exception might be a willingness to force the tiny sliver of wealthy seniors to pay more in Medicare premiums. The wealthiest 2% of seniors already pay more for their Part B and Part D premiums but everyone gets Part A (hospital services) for no premium as that portion is financed by the Medicare portion of FICA payroll taxes – 2.9% of all wages with no cap nominally split evenly between the employer and the employee. Starting in 2013, there will be an additional 0.9% Medicare tax to be paid on the portion of income, including investment income, for single taxpayers above $200K and married couples above $250K.
By the way, Medicare is already, in effect, a single payer system for the population it covers as even Medicare Advantage insurers generally also reimburse providers at Medicare rates and sometimes even less. The record on cost control is unimpressive to put it mildly while fraud is likely quite significant but not precisely quantifiable.
“So are you planning on running for office on that platform? How sucessful do you think you will be?”
Are planning on running on a platform of single pay?
Legacy, an average is the lows and highs combined, I suspect MD is in a region of high wages, unions, high rents, home prices and taxes – one of the highs. If it were low then it would be harder to get below average because the average would also be lower. It would also be harder to competent with surrounding states.
“The Government is a big dumb animal.”
“Yes:
– Single payor
– Tort reform
– “Death Panels” – yes I believe there needs to be someone who represents the state/taxpayers involved in the decision to “unplug Grandma””
I think single pay means more government. I also think single pay is the only path to better cost control, however I don’t think tort reform is part of the answer as in states with it their costs are not lower. It’s really a red herring.
As for some sort of government plug pulling I worry about the slippery slope. Government may be able to control the purse, but health decisions should be between a doc and you. I have a health directive that does not involve heroic methods, I think most people would do otherwise if encouraged.
P.S.
Most of the Imaging Centers are NOT hospital owned. Frequently they are “joint ventures” to which the hospital has contributed NO MONEY, but still receives revenue from.
Bob,
“The solution is to have a Medicare Czar who has only one duty — to come under budget for the year. He would ignore hospital protests……
He would say, “Cut your costs, Mr/Mrs Hospital, or drop out of Medicare. We do not need you that badly.”
Seniors might have to drive 50 miles for discretionary surgery. Given the massive subsidies that seniors receive, big deal. Cost control is not a beanbag.”
So are you planning on running for office on that platform? How sucessful do you think you will be?
Barry,
Correct with respect to imaging centers. Many of these are located on hospital campuses in “unregulated space”. This means that severely ill patients have to be transported by ambulance – sometimes even less than 100 yards. Thank you HSCRC! And if they were regulated on campus the owners would merely buy real estate off campus which would change the ambulance ride from 50 yards to 300 yards.
Maryland is a high cost state – check it for yourself. I don’t know if utilization is above average or not. You assume because it is HSCRC regulated per procedure costs are lower – why do you assume that? The HSCRC creates rates that keep hospitals alive. Get your gallbladder taken out at Hopkins and pay almost twice what you pay at some other hospitals in the metro area.
Maryland has NOT been successful at controlling costs. The HSCRC has been in existence for over 30 years, Maryland remains a high cost state. If I were in another State or working for the Feds I would NOT follow Maryland – unless I were someone who liked government control in and of itself – which many people who read this blog do.
Peter 1,
With respect to the Dartmouth data I think it is very useful and should be looked at carefully. The problem is – what conclusions do we draw from it and how do we put those into action. I definitely believe that there is over treatment / over diagnosis going on in the US – I see it every day. However one man’s over treatment/ over diagnosis is another man’s “just right” (like the 3 bears).
Where would Maryland need to be to be a low cost state? Below the national average instead of above. (that was an easy one)
Is there anything you like?
Yes:
– Single payor
– Tort reform
– “Death Panels” – yes I believe there needs to be someone who represents the state/taxpayers involved in the decision to “unplug Grandma”
In essence a system like the Canadian or British system.
My understanding is that while reimbursements are lower in Maryland, the number of admissions has increased.
To use a crude example, say you have 1,000 admissions paying $17,000 each in year 1.
In year 2, an aggressive insurer (or Medicare) lowers the reimbursement to $15,000.
But suddenly you have 1,200 admissions. Total expenses for the insurer are $1.8 million versus $1.7 million under the old regime.
According to Joseph White, who is my guru on these matters, Germany had exactly this problem in the 1990’s.
The govt responded by paying only 25% of the standard fee on any admission over 1,000.
This is classic cat and mouse, nothing revolutionary.
American Medicare is just totally timid in these areas.
The reason, I think, is that American Medicare does not have a hard budget.
And simple administrative initiatives have to be approved by Congress.
The solution is to have a Medicare Czar who has only one duty — to come under budget for the year. He would ignore hospital protests.
When a hospital says, you are not covering our costs, he would respond the way that Walmart does to a vendor who cannot survive on what Walmart pays for toothpaste. He would say, “Cut your costs, Mr/Mrs Hospital, or drop out of Medicare. We do not need you that badly.”
Seniors might have to drive 50 miles for discretionary surgery. Given the massive subsidies that seniors receive, big deal.
Cost control is not beanbag.
Sen
Correction: First paragraph should read 100 or 200 yards by ambulance, not years.
“It has also pushed many procedures out of hospitals into “imaging centers or surgicenters””
Legacyflyer –
If I remember correctly from the discussion several years ago, some of these imaging centers and surgical centers are located on hospital campuses and owned by the hospital but they’re considered “unregulated space.” So, you sometimes have the ridiculous scene of a patient being transported 100 or 200 years by ambulance from his hospital bed so he can have an image or a surgical procedure done in (price) unregulated space.
Second, if MD is indeed still a relatively high cost state, it suggests that utilization is above average as well so providers can make up any underpayments with higher volume. To maximize reimbursement in a regulated environment further, there may be more upcoding as well. Might this be the case in your experience?
Finally, even if MD were successful in mitigating cost growth with hospital price regulation, it’s doubtful that other states could copy it today even if they wanted to because Medicare and Medicaid would have to agree to pay higher reimbursement rates than they do now so private insurers could pay less. That’s not likely to happen given the fiscal challenges at both the federal and state levels.
Prior you seemed to question the usefulness of Dartmouth study, now you reference it?
Where would Maryland need to be to be considered a “low cost” state?
“Your remedies are the standard ones; an appeal to “providers” to be good girls and boys and “choose wisely” about tests and treatments and a faith that ACOs will solve the problem.”
“you like regulation despite the fact that it has not been effective.”
Is there anything you like?
This reminds me of a “discussion” I had with Maggie Mahar several years ago.
For those who think that the HSCRC has been effective in controlling costs go to the colored chart in the prior article: “What Does the Dartmouth Atlas Have to Say About the Politics of the ACA” by ANUBHAV KAUL, MD, et al – and look at the color of Maryland – dark green = highest cost. Or go to the Dartmouth website.
What the HSCRC has done is to keep Hopkins (and U of MD) in fairly good shape by forcing insurers to pay higher rates to these institutions. (and they probably deserve it for all the indigent care and research they perform) No surprise that Gerard Anderson likes it.
It has also pushed many procedures out of hospitals into “imaging centers or surgicenters”
What it has not done – over the course of more than 30 years – is to make Maryland a low cost state.
You and Maggie both seem to prize form over function – that is – you like regulation despite the fact that it has not been effective.
“So your solution to dying an agonizing and expensive death is to cut reimbursement to hospitals for ICUs?”
“agonizing” – drugs
“expensive” – health care directive
“Maryland is a fairly high cost state and cost growth has paralleled other states.”
Is this a false statement?
“No insurer wants to be known as being obsessively aggressive against price increases,” said Gerard Anderson, director of the Johns Hopkins University’s Center for Hospital Finance and Management. “If you’re an insurance company, you stand to lose a large client [the hospital] all to gain a small rate reduction.”
Anderson argues that stronger government intervention is necessary to slow price growth in the health-care market. He points to the example of Maryland, the only state where the government sets the rates that hospitals can charge insurance companies.
The program began in 1976, when Maryland’s per-admission hospital spending was 26 percent higher than in the rest of the country. Between 1977 and 2009, the state’s hospitals “experienced the lowest cumulative increase in cost per adjusted admission of any state in the nation,” researchers in the Journal of American Medical Association concluded.
“Hospital prices have been held down substantially,” Gerard said of the Maryland experience. “And private insurers pay the same rates as public insurers.”
Such efforts, however, have fallen out of favor in other states. Congress gave states the authority to set payments in the early 1970s. About 30 states went on to do so. All states except Maryland gravitated away from those models, as states have looked for more competition and less regulation in health-care markets.”
So your solution to dying an agonizing and expensive death is to cut reimbursement to hospitals for ICUs?
My state (Maryland) has a cost review commission that controls all hospital rates. The results are not impressive – Maryland is a fairly high cost state and cost growth has paralleled other states.
To someone with a hammer, everything looks like a nail.
Republican solution for pension costs – die young
Republican solution for health costs – die quick
Unless of course they want to win an election, then it’s “death panels” where they want endless money spent on the near dead.
“But from what I have read about Canadian and German health care, this sort of cat and mouse conflict goes on all the time in those countries.
Health care cost control is an endless struggle…”
Yes it is.
In the last year I had two close friends who died agonizing deaths.
Financially, the huge charges to Medicare mainly came from daily ICU reimbursements. (There were no heroic surgeries.)
In strict budget terms,, we could start to fix that tomorrow morning. Just reimburse hospitals at $1500 a day instead of $5,000 a day, and bundle the fees.
Any doctor visits or blood tests would have to be paid out of the $1500.
Now this would start a whole series of counter moves by hospitals to keep people in the ICU for an extra week, or to find some procedure that can be charged at full price, etc.
But from what I have read about Canadian and German health care, this sort of cat and mouse conflict goes on all the time in those countries.
Health care cost control is an endless struggle against providers who want to preserve their high incomes, and for that matter to just meet their monthly expenses for rent, staff, and malpractice insurance.
Rather than shy away from such conflict, we should see it as inevitable and just wade in if we want to control costs.
We learn of new flaws and hidden expenses nearly every month of late. Hmm, if this legislation was just 900 pages and easy to digest, why all the surprises that keep surfacing? Oh, yeah, politics.
Lots of “i”s in that word, don’t find them in the words “health care”, eh?
Just like the word “team” is as foreign in DC these days too?!
Run, do not walk to the nearest exit. And I like your end comment of the above as well.
Gee, who is paying that increase? Ah, yeah, you and I and the rest of the suckers who stay in the US and allow the ongoing taxation without representation to continue.
New irony to the adage “the more things change, the more they stay the same”, or, more recently by Pete Townsend, “meet the new boss, same as the old boss”. King Barack really has you all awed and awful, eh?
The amount of spending on “late-stage, Hail Mary” treatment is HUGE.
The chance of getting a politician (Democrat or Republican) to step anywhere near this “death panel” issue is TINY.
That is why we are “re-arranging the deck chairs on the Titanic”.
On my recent hospital stay in India it was 2 nurses for every patient, or so it seemed – great service, push the call button, no waiting.
Of course nurses there are low pay, as well I was cash pay. What I did notice was the tremendous attitude toward customer service throughout the hospital, no matter what the ability or method of pay. Hospital was extremely busy, much more than any U.S. hospital I’ve been in.
Bob –
There was an article by health policy expert and oncologist Ezekiel Emanuel in yesterday’s New York Times which expressed considerable skepticism about the potential to save significant amounts of money on less futile and inappropriate end of life care though I think there is probably somewhat more potential than he claims. He noted that the 6% of Medicare beneficiaries who die each year account for 27%-30% of Medicare costs in that year. However, that ratio has been about the same for many years.
I thought rbaer’s comments yesterday in response to my questions about hospital costs and staffing were very informative. He noted that we provide more intensive care than in German hospitals, we have a greater margin of safety built into the system, there is more staffing on weekends, doctors make more money in the U.S. than in Germany, patient expectations are higher in the U.S., there is more paperwork and bureaucracy here and patient expectations are higher and less forgiving. Moreover, drug and device prices are far higher in the U.S. than elsewhere. It all adds up. The litigation environment in the U.S. also contributes to more testing and higher costs. The cultural aspects of all this won’t be easy to change. At best, it will take a long time.
As it relates to end of life care specifically, however, I do think there is a lot more that we can do to greatly increase the percentage of elderly people who execute a living will, advance directive or POLST and make sure the information is stored on a registry so it’s available to doctors and hospitals when needed. A $10 per month surcharge on the cost of Medicare Part B premiums for those who don’t execute one of these documents would help prod them to do so, I believe.
Regarding Barry’s comments on Medicare…………..
it would be interesting to know how much Medicare spending goes to hugely expensive and late-stage Hail Mary treatments for cancer and organ failure –
versus the more prosaic but also more numerous treatments for just the normal parts of growing old — hip and knee replacements, memory loss, pneumonia, digestive ailments, eye surgery, etc.
I used to think that if we somehow cut back on heroic treatments, which involves accepting death, then we could save Medicare fiscally.
But I am starting to wonder. I have no access to Medicare claims data, but someone does and I would like to know of any studies in this area.
Thanks rbaer. That’s a very informative summary and analysis.
From my residency years at several hospitals in Germany, I can tell you: RNs and in particular docs are better paid in the US – hospital docs in Germany are really underpaid and the country notices that their docs are migrating (mostly England, Switzerland), some of the voids filled by eastern European docs with limited German skills). In the US, drugs and devices are insanely overpriced (in germany only moderately so). The intensity of care and of staffing is much higher in the US. If a German nurse has, say, 8 patients, only 1 or 2 truly need attention, while a US RN may have only 2-4 patients, but more more active ones … and much more paperwork. And since hospital stays in the US are so short, more weekend coverage from techs and therapists are needed (at least in larger hospitals), while really not much is going on in German hospitals on weekends unless it is a true emergency. In general, german hospitals are more lean, much less bureaucracy, discharge planning, coding, slimmer safety margin, less supportive staff, at times inappropriate (I worked in a psychiatric hospital that was operating extremely leanely at night – 8 wards with 30 patients in a high rise, if someone became violent and needed fixation/drugs, the 2nd person from each ward helped out when activated by phone from the ward in need, no security, no labs at night – if needed, patients were transferred).
” It can’t all have to do with fear of litigation and patient expectations.” Culture/slowly developing customs and standards play a role as well. German patients demand less, on average, less pefection, and understand that residents, students, student nurses have to learn and are not perfect. A german hospital day rate for EVERYTHING was (of course, that depends on hospital type), if I recall correctly much less than just room/board/nursing in the US (now DRGs are used in Germany so the daily rates are irrelevant).
The inability of CMS to maintain physician income increases inline with inflation or medical inflation has resulted in an ongoing squeeze-play of declining margins, and in many situations, unsustainable financial viability. Thus out of necessity, the logarithmic increase in health system/hospital physician employment will continue, whereby very few if any practices will remain independent.
To Dr. Wes’ point, and contrary a few of the comments here, any impact on hospital-side reimbursement will therefore impact physicians both directly and indirectly. No real ‘fix’ here.
That’s scary
“The ACA is probably one of the most complex rearrangements of the deck chairs on the Titanic one could imagine.”
__
Imagine. You and I agree on something.
President Obama for his likely signature.
The Government is a big dumb animal.
Our nation is like a family that is spending too much on food. We buy staples like potatoes, vegetables and bread. We also buy “luxury items” like Champagne, imported cheese and caviar.
The rational solution to the family’s problem with its food budget would be to cut back on the Champagne, imported cheese and caviar, but continue buying staples. The government solution is to cut everything 10% – including the potatoes and vegetables.
Similarly we spend too much on health care including primary care, pediatrics and other basics as well as the “luxury items” of liver transplants, futile chemotherapy and ICU hospitalization during the last weeks of life.
Rather than targeting the “luxury items”, the government just cuts everything some percent. This is called a “fix”
The ACA is perfect example of such a “fix”. The ACA is probably one of the most complex rearrangements of the deck chairs on the Titanic one could imagine.
Bob –
When the ICD-10 hospital coding system is finally implemented and supplants the current ICD-9 system, the number of codes will expand by at least fivefold. While this will have some benefits for academic researchers, it could also easily lead to even more upcoding.
My understanding is that healthcare payment policy in other countries is driven primarily by trying to pay for necessary care and not pay for unnecessary care. By contrast, Medicare’s underlying approach is to cover provider costs. If costs are driven up by inefficiency and/or providing lots of unnecessary care, it still seems to get built into the cost structure that gets reimbursed. New drugs that win FDA approval are generally paid for even if they are no more effective but much more expensive than competitive therapies. They just have to be more effective than a placebo to win approval.
Since we are not likely to change this culture anytime soon, I would prefer to attack costs through such strategies as litigation reform, especially safe harbor protection for providers who follow evidence based guidelines where they exist and monthly surcharges for Medicare beneficiaries who have not executed a living will.
The program should be restructured in a way that provides a range of unified deductibles from a minimum of $1,000 to a maximum of at least $10,000 regardless of whether the expense is for a Part A or a Part B service. There should also be 20% co-insurance above the deducible with an out-of-pocket maximum amount of between $5,000 at the low end to $25,000 at the high end. The Part D drug benefit should be revamped along the same lines. Raise the deductible at the low end, provide a reasonable OOP amount at the high end and eliminate the donut hole. People who want to can buy supplemental policies to cover most or all of what Medicare doesn’t pay for.
Reference pricing might also be helpful. That is, if proton beam therapy for prostate cancer is currently reimbursed at over 50% more than the more standard IMRT but is no more effective, we shouldn’t pay any more for proton beam than we do for IMRT. Patients who want proton beam can pay the difference out-of-pocket and not have it count toward their deductible or OOP maximum. Of course, that difference is currently about $13,000 which not many seniors can afford but why should taxpayers cover it?
Finally, go after fraud with all of the state-of-the art analytics that we have and employ private contractors to help.
A faster way to cut down on hospital upcodings would be to wipe out the higher-paying codes.
In other words, if a heart failure case has 3 DRG codes, wipe out the top one which pays the highest.
Then you have to worry about increased utilization, as hospitals try to make it up in volume.
You could deal with that by withholding 10% of every single reimbursement until the end of the fiscal year, to be sure you do not go over budget.
These are old hat techniques in Germany, Japan, etc. American Medicare will probably take years to come around to them, because Congress is so dependent on contributions from health care providers.
As for the doc fix and related issues, it is somewhat absurd for Medicare to be paying any claim under $500. People under 65 bear up with $300 medical bills with or without health insurance every day of the year, but a $300 bill to a non-poor senior citizen is considered a national emergency.
The solution to Part B upcoding is to give each senior a prepaid debit card for $1,250 or whatever for office visits. The doctor can charge what they please, and be paid in 30 seconds when the card is swiped in their office.
If a senior is spending more than $1,250 in office visits, one can assume there is price gouging going on somewhere.
Bob Hertz, The Health Care Crusade
May I offer a bit of good news in all this gloom. Per the ACA, in 2013 and 2014 Medicaid fees for primary care must be no less than 100% of Medicare fees. In my state (CT) Primary Care physicians will see increases of from 70% to 136% in their fees for treating adults on Mediciaid and increases from 6% to 53% for treating kids under age 19 on Medicaid. The fee for the most commonly billed office visit (99213) for an adult wil go from $37.48 to $77.93, an increase of 108%. Medicaid will now pay more han many of the largest commercial insurers for many primary care services in certain plans. This will go a long way to increase access to primary care services for this population.
I would still like some insight regarding why U.S. hospitals’ prices per service, test or procedure and their costs, especially related to the number of employees per licensed bed, are so much higher than for similar hospitals in other developed countries.
The weird thing is that hospital inpatient bed days per 1,000 people in the U.S., the average length of stay, and the number of discharges per 1,000 people are all below the OECD median according to the Kaiser Family Foundation. Most hospital bed days are accounted for medical as opposed to surgical patients so the medical arms race in operating rooms is presumably not a dominant factor driving costs. I don’t think higher physician compensation compared to doctors in other countries is a significant cost factor either. Are we performing way more tests per patient and, if so, why? Are we administering more drugs and more expensive drugs and, if so, why? Most importantly, why are there, apparently, so many more employees per licensed bed in U.S. hospitals? I’ve never heard a good answer. It can’t all have to do with fear of litigation and patient expectations. Could it?
I’d rather rob Peter and Paul to lower costs.
Pitting the American Medical Association (AMA) against the American Hospital Association (AHA) is one way to reduce healthcare costs, IMO. So, if robbing Peter (i.e. the hospital) to pay Paul (i.e. the doctor) will significantly lower the overhead or administrative costs in hospitals, I’m all in favor of it!
“(You well-paid primary care doctors, are you listening?)”
Maybe, but I bet those really high paid specialists (like yourself) are.
So Doc Wes, what is your fix seeing that we pay the highest prices in the universe?
I would add that the “fix” is an adjustment of zero percent, which is better than a reduction of almost one third, but hardly a “fix” because there is surely positive price inflation to physicians’ practice costs. Original SGR “fixes” increased the adjustment with practice costs but this stopped a while back.
While the pure SGR reduction would be catastrophic, a “fix” of zero percent is more like a frog in a pot of water slowly coming to a boil. However, until the medical community accepts a Republican-style reform of making the taxpayers’ contributions a defined contribution, physicians have no hope of getting back the ability to balance bill.
The rational response by physicians to this is to see more healthy Medicare patients for very short appointments, check the right boxes, and make up their revenue on volume. Not a good incentive, I trust we’ll all agree.