 In our rush to establish a national electronic medical record (EMR) system as part of the American Recovery and Reinvestment Act of 2009, powerful silos of independent EMR systems have sprung up nationwide.
In our rush to establish a national electronic medical record (EMR) system as part of the American Recovery and Reinvestment Act of 2009, powerful silos of independent EMR systems have sprung up nationwide.
While most systems are being developed responsibly, like the Wild, Wild West, many have been developed without an objective eye toward quality and the potential harm they may be causing our patients.
As most readers of this blog are aware, since 2005 the medical device industry in which I work has had widely publicized instances of patient deaths splashed all over the New York Times and other mainstream media outlets from defibrillator malfunctions that resulted in a just a few patient deaths.
The backlash in response to these deaths was significant: device registries were developed, software improvements to devices created, and billions of dollars in legal fees and damages paid to patients and their families on the path to improvement. In addition, we also learned about the limits of corporate responsibility for these deaths thanks to legal precedent established by the Reigel vs. Medtronic case.
Should Electronic Medical Records Be Considered Medical Devices?
I received a medical record from a large academic medical center somewhere in the United States (the details are unimportant) that has one of these new pioneering EMR systems manufactured by $13 billion-dollar company, Cerner Corporation. Now before I go on a rant about Cerner’s EMR system, I should preface my remarks to say that I have never personally used Cerner’s system. But I am a doctor who received a note composed on Cerner’s system and what I saw was one of the better examples of how EMRs are contributing to misinformation and confusion when health care is delivered.
I received a copy of an internal medicine consult that was performed on a patient at this outside hospital. I have extracted the “medications” portion of the internist’s note exactly as it was displayed in the note below (although the list extended over more than one page, so I joined the list together as one figure). Needless to say, I was terrified at what the system had listed as the patient’s medications:
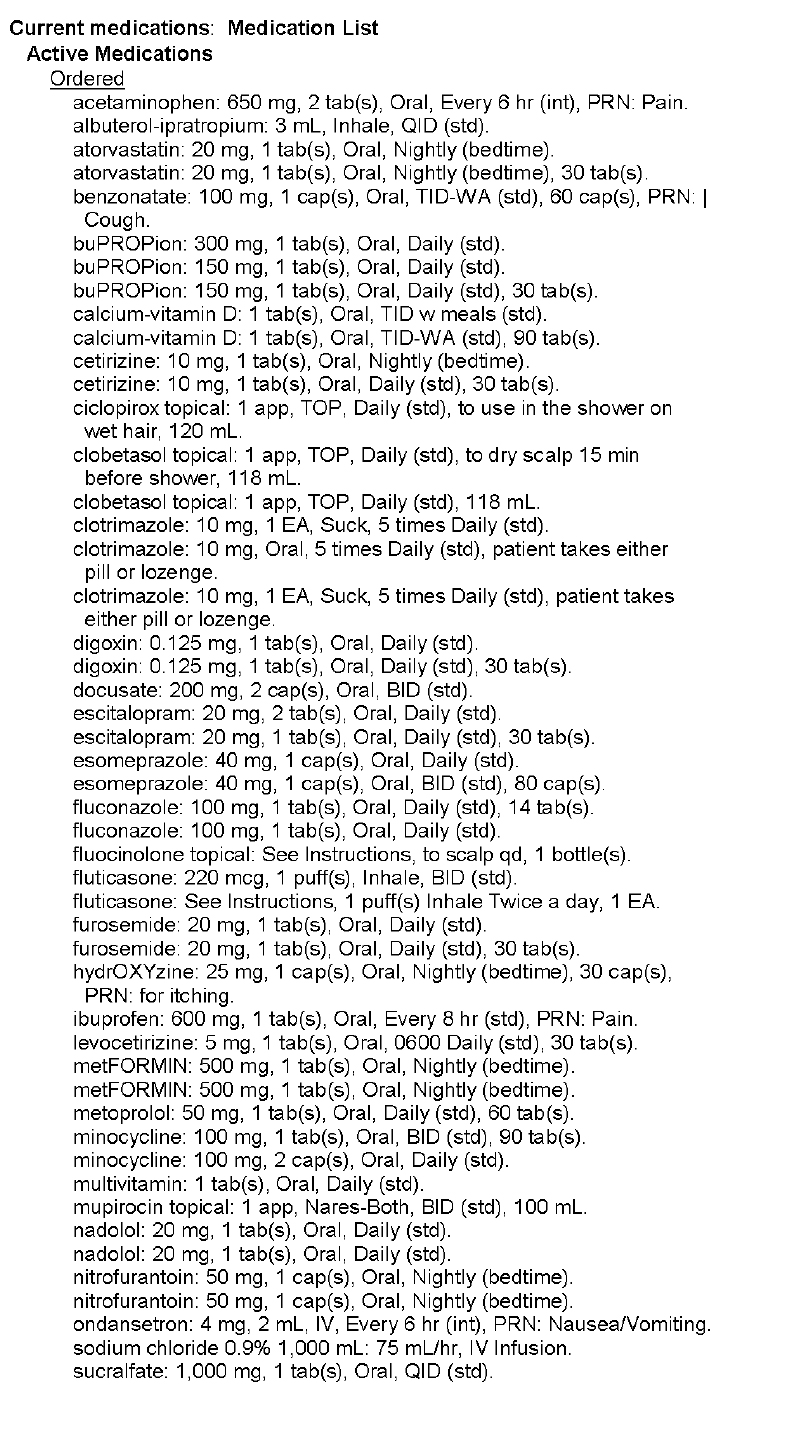 |
| Med List (Page 1) – Click to enlarge |
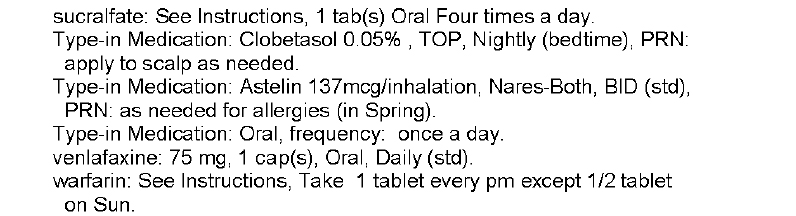 |
| Med List (Page 2) – Click to enlarge |
In this example, we see multitudes of medications listed more than once. We see drugs of similar classes (antihistamines, beta blockers) on the same list. We see warfarin, one of our most dangerous drugs dispensed, without a dose included. We see what seems to be outpatient meds listed with inpatient meds, I’m not sure. Honestly, we really have no idea what medications are actually being taken from this list. And yet this list of medications is listed by the EMR as the patient’s “Active Medications.”
What the heck have we created?
Certainly, any capable physician who cares for patients would describe this medication list as worthless. So why is it in there? (Don’t get me wrong, the fact that any doctor would allow such crap to be displayed in his or her medical note by using an EMR shortcut to enter them uncorrected is beyond me. Certainly, we as doctors must accept a big portion of the responsibility for this).
But when EMR developers and their hospital administration customers purchase software capable of spewing forth completely useless AND potentially lethal information about our patients that is then transmitted far and wide, (not to mention to local direct caregivers) doctors have an obligation to speak up.
These kinds of documentation problems are the EMR’s Achilles’ heel. But beyond this, EMR software updates are routinely deployed without real-world real-life testing. Ever. And yet, like patients with a defibrillator who die outside the hospital before a root cause of a defibrillator defect can be discovered, I acknowledge that it is incredibly difficult to prove that the death of an individual was caused by an EMR software problem.
And yet, we must.
So how will we measure problems with EMRs? It seems industry representatives would rather not address these concerns. We should ask ourselves, is anyone thinking about this?
Right now, the prevailing belief is that the electronic medical record might be one of the most important medical devices doctors have at our disposal to care for patients. I tend to agree. But it’s potential to do harm is also enormous if it is not used responsibly and accurately. After all, as the above example shows, the potential to introduce unintended yet potentially lethal errors into patient care is huge. More importantly, since nearly every person in the United States will soon have their medical data housed within these systems, the number of people that could be adversely affected by these systems is much larger than what we’ve seen with our recent defibrillator malfunctions.
Perhaps, like the ICD registry, we should try to to develop an EMR registry of adverse patient outcomes caused by these software systems. That way, every independent EMR company can learn from the other’s mistakes. Because, guess what …
… like other man-made medical devices, EMR’s are not perfect either.
Westby G. Fisher, MD, (aka Dr. Wes) is a board certified internist, cardiologist and cardiac electrophysiologist practicing at NorthShore University HealthSystem in Evanston, IL. He is also a Clinical Associate Professor of Medicine at the University of Chicago’s Pritzker School of Medicine. He blogs at Dr.Wes, where this post originally appeared.
Categories: Uncategorized








Really a good article. I appreciate it.
Top emr software companies
The records can only be as good as what information the person putting the information in. Don’t think it is the software per se. It is how it is being used.
hi!,I like your writing very a lot! proportion we keep up a correspondence more about your article on AOL? I require a specialist on this area to resolve my problem. May be that is you! Taking a look ahead to peer you.
You are correct – I’m guilt of hyperbole. EMRs do indeed reduce the productivity of healthcare, increase it’s costs, and produce minor effects, both positive and negative, on some aspects of actual patient care. These do qualify as “whits” – but not “meaningful whits.”
Working as an informaticist and a practicing physician, I am well read in the literature of medicine, HIT, and IT. As was the case in the past with global warming, 2nd hand cigarette smoke, HIV/AIDS and alternative energy, the literature of the field is highly politicized/polarized and, in some cases, extremely biased. Interestingly, the conclusions of the periphery of HIT – in medicine and in IT – tend to be less so, but any article I read emanating from the government or the HIT industry specifically I tend to regard with great skepticism. The headlines are often based on some particular point that the author is trying to prove, and the references range from useful to specious.
With the financial stakes as large as they are this is inevitable to some degree, but the government’s deep involvement in this particular problem presents, once again, as the root cause of the many problems HIT faces that I pointed out in my original post.
The pattern is beginning to appear again in diet and nutrition. As the diet modification industry grows, watch for the same effect. Once you learn to recognize the patterns, it is surprising how often one finds them repeated.
Sure there are systemic issues that need to improved, and I’ll defer to your local knowledge on what these problems are in the US, but your later point that EMRs “don’t affect [healthcare] one whit” is uniformed, and is a meme which is being spread irresponsibly.
Take a look at the literature – there are innumerable documented studies of many “whits” of positive impact. However the fact is that the software and the implementation are critical to achieving this benefit. Just installing a system doesn’t cut it.
What you see in the above example is as much a problem of the end user as the software. Obvioulsy this patient has an unmaintained active meds list, nurses and physicians or whoever have been blithely placing those orders and NOT looking at what they are still on. Garbage in, Garbage out. What this show is that our electronic records need to be as actively maintained as our old paper ones. there seems to be some belief that the EMR atuomagically makes all things better, it doesn’t. Blame ourselves as much as the software. We still need to do the work. (and don’t discount the importance of training).
This is a big issue, Bob, that I think the provider community should address. Can’t some of the professional organizations (such as AMA) take this on and demand better accountability? This is important not only because physician liability is increased, but because patients could be harmed. I can see there’s a catch-22 – you have to get an EHR system for your clinic or hospital, but you bear responsibility if it fails. Yikes!!
I agree, doctors and nurses need to be able to read patient records on the move. Technology these days doctors and nurses can do this.
I have just completed two month of owning of Samsung Galaxy Nexus and I have no doubt declaring I am very happy with this. This is the best smart phone on the market for the time being until iPhone 5 or Samsung Galaxy S3 releases. I had iPhone 4 for 2 months and I like many other people who could not be satisfied with beauty and fruit brand alone threw that dumb beauty’ . For me that was more of a show off’ rather than of practical use.
Outstanding article but, like most responders, I disagree with your solution to the problem. And I question whether you’ve identified the correct problem, i.e. the “root cause” we hear so much about.
EMRs suffer from inherent weaknesses – they are notoriously complex, they are a drag on productivity, their business case is very, very weak, and they are enormously expensive to both purchase and support.
Piled onto those problems, which were enough to prevent widespread industry adoption until 2009, the government has now mandated them. And THAT is the root cause of the problem.
Because of government mandates, hospitals no longer have the option of waiting for a better product. Because of the mandates, product improvement has been shelved or severely curtailed as vendor resources have been sucked into Meaningless Use requirements. Because of the mandates, many billions of dollars have been diverted from patient care to what is, essentially, payer care. Because of the mandates, vendors can use contract language which absolves them of any liability for the use of their products. And, because of the mandates, you have received a page and a half of more or less worthless and potentially dangerous information about one of your patients.
But what are our options?
Doctors dare not complain about the systems in any meaningful way, such as refusing to use a dangerous product, because of – you guessed it – government mandates. The Joint Commission, which has what amounts to law-writing capability by virtue of how they were legislated into symbiosis with CMS, has deemed that such forms of resistance to EMRs can be deemed “disruptive”, and a physician so labelled will never work again because of – once again – the government mandated National Practitioners Data Bank, which ensures that such a label will be inescapable, un-appealable, and immune from rebuke.
Hospitals cannot refuse to comply, as it will cost them a large portion of the revenue from their single biggest payer, not to mention that in doing so they will bring upon themselves the full wrath and fury of every government inspector from OSHA to CMS’s Civil Rights office to RAC audits.
Patients can’t help us – most don’t know anything about EMRs, many that do don’t care, and the few that remain are subjected to a constant bombardment of government and industry propaganda telling them the EMRs will _improve_ their health care. I have yet to see a mainstream story which delineates the difference between health care, which EMRs don’t affect one whit, and health care documentation, which EMRs at least have the potential to improve.
Having said all the above, I’m compelled to point out that I’m a supporter of the _concept_ of EMRs, and I work in the industry.. By improving documentation, they offer the opportunity to make more data available, faster, to those who actually provide health care. By aggregating documentation, they offer the potential to allow medical researchers to spot heretofore undiscoverable clues affecting the treatment and management of patient populations. But in their current state of development, they’re garbage.
Worse, they’re just one of many piles of garbage forced by the government upon what was once the world’s greatest health care system, all in the name of “reform.”
Oh! This blog is really a great collection of facts. I actually dint know this much about EMRs. Having gone thru this article I have understood that EMRs can definitely aid to medical practice but has a terrible mirror image too. Medical field is a real sensitive field where one small error could lead to fatal outcomes. One spelling mistake can mean a life at stake. I am under no circumstances ready to vote for such a system to be a part of medical industry.
The specific issue cited with the Cerner hospital EHR shows how the vendor has confused a prescription list with a medication list. The deeper question is whether federal regulation or market pressure should be the motivator for change among EHRs. And who should do the regulating? The IOM has looked at this extensively, and has concluded that it should *not* be the FDA (who has wanted to regulate EHRs as medical devices). Perhaps hospital EHRs should be viewed differently than ambulatory EHR, for a variety of reasons.
These quesitons are probed more deeply in an article I wrote here: http://robertrowleymd.com/2012/06/07/what-motivates-an-ehr-to-change-and-improve/
EMR what an incredible hassle for independent offices. My software is now compatable with all the government rules but what is the reason for all of this. We have taken a system that was not broken and created another system so complecated that its hard to believe that it will ever work. In the past if you needed recors you had them in a day or two. How is this better, a massive amount of data thats hard to pick through. Thanks for the great blog.
Dr. Wes, thoughtful post on an important topic. Not sure where I come down yet on the regulation question and who is best to police these “product liabilty” type questions. I will bring to your attention another issue that I see as a health care attorney who regularly gets to review software/hardware vendor agreements for leasing, purchasing, using, etc. EMR systems. The Limitation of Liability sections of these standard boilerplate software licensing agreements push any and all liability for the failure of these systems back on the health care provider – whether hospital or physician. In additional to limiting direct liability for any loss or damages they often include provisions that also limit the amount of damages. These very one sided provisions are very difficult to negotiate away from in the midst of working through reaching an agreement. Health care providers are typically at a disadvantage in the negotiation process on these issues. Thanks again for the interesting post. Bob
Physical records usually require quite a lot of space to keep them. When physical records are no more maintained, the big levels of space for storage are no more needed. Paper, film, along with other costly physical media usage can also be reduced with electronic record storage
So the electronic EMR is an adjunct to, not the replacement for, a good medical history. Unless the patient is an unconscious trauma victim, most people should be able to answer a simple question about a doubtful entry in an EMR.
I agree with Sandra – the health records belong to the patient and it is the patient’s responsibility to make sure they are right.
That said, the medical information companies need to keep it reasonably easy to peruse. ( Unlike the tax code)
The only way for healthcare information to be accurate is for patients and their proxies to make sure it’s so. Mistakes happen, and systems (like Cerner’s) are not likely to be able to fit all needs. So just like you check your banking statements, you should be able to check your basic health records.
This is an interesting post, thanks for sharing.
It’s without question that the potential for error is significant with serious consequences. But if EHR’s are to become regulated like medical devices, what would it look like?
Do you think they would be subject to significant oversight given they are equally important as surgical mesh etc.? Would they be subject to the device tax set to take effect in 2013?
Here’s a look at how the taxes on med devices in the U.S. shakes out: http://americanactionforum.org/topic/economic-impact-medical-device-excise-tax
The ONC EHR Certification program is pretty feeble.
http://clinicmonkey.blogspot.com/
I have encountered a number of “certified” systems that simply do not work as advertised. I keep thinking “how the [bleep] did you pass CHPL”?
(Asked and Answered)
Good points and observations about the dangers of EHR.
But I’m not convinced that regulating EHRs as medical devices is the answer.
First, we have, as a nation, committed time and resources to the process of certification of EHRs. The certification process is focused and specific to EHR. I’d rather see us improve the processes and standards attached to this than to add a redundant and non-specific bureaucratic burden to the process.
Second, there remains a lack of “artistry” in the creation of EHR documentation. Remember the “Art of Medicine”? The EHR represents the science. But, as with all tools, the science takes us only so far. Perhaps a great EHR, someday, will create a great note out of any garbage I input. But for now, there is an opportunity to make better EHR notes by promoting the art of EHR notesmanship.
We all trained with masters of the narrative summary. As a result, most of us are reasonably good at the narrative summary. But we don’t have, yet, masters and role models of the ideal EHR documentation/note. We need examples of good and bad notes. We need to be made aware of how our inputs are seen by the consumers of our documentation and how we effect, by our inputs, the quality of our outputs. We need training and feedback about the quality, or lack thereof, or our notes.
Though I see value in improving the technical issues of certification standards and the processes around setting, implementing, and monitoring those standards, I think we are neglecting the human side and must promote artistry and responsibility in our EHR notesmanship.