We’ve been duped! Everyone said nothing’s been going on in digital health, but Amazon bought OneMedical! Keep watching for our thoughts and new deals: Cleery raises $192 million; Health Note raises $17 million; Elation raises $50 million; Caraway raises $10.5 million.
This was a special early in the day edition of #THCBGang. It was at 9.15am PT/ 12.15 pm ET (so if you are coming at 1pm it won’t be live today at the normal time as it’s already happened!). It was part of the Primary Care Transformation Summit which has been running since Monday and continues to the end of Friday. It’s a who’s who of everyone in primary care. You can check out the wider agenda but we were on immediately before the day 3 keynote from head of CMS Innovation, Liz Fowler.
Joining Matthew Holt (@boltyboy) to discuss primary care and more were are WTF Health host & Health IT girl Jessica DaMassa (@jessdamassa); futurist Jeff Goldsmith; & Dan O’Neill (@dp_oneill) who is now at primary care group Pine Park Health.
You can see the video below & if you’d rather listen than watch, the audio is preserved as a weekly podcast available on our iTunes & Spotify channels.
July 25, 1972 was fifty years ago this week and it is a day that all AP Science journalists know by heart. As Monday’s AP banner headline read: “On July 25, 1972, Jean Heller, a reporter on The Associated Press investigative team, then called the Special Assignment Team, broke news that rocked the nation. Based on documents leaked by Peter Buxtun, a whistleblower at the U.S. Public Health Service, the then 29-year-old journalist and the only woman on the team, reported that the federal government let hundreds of Black men in rural Alabama go untreated for syphilis for 40 years in order to study the impact of the disease on the human body. Most of the men were denied access to penicillin, even when it became widely available as a cure. A public outcry ensued, and nearly four months later, the “Tuskegee Study of Untreated Syphilis in the Negro Male” came to an end.”
The New York Times had an interesting set of op-eds last week under the theme “I Was Wrong.” For example, Paul Krugman says he was wrong about inflation, David Brooks laments being wrong about capitalism, and Bret Stevens now fears he was wrong about Trump voters. Nobody fessed up about being wrong about healthcare, so I’ll volunteer.
I’ve been writing regularly about healthcare for over a decade now, with some strong opinions and often with some pretty speculative ideas. I’ve had a lot to be wrong about, and I hope I will be wrong about many of them (e.g., microplastics). Some of my thoughts (such as on DNA storage or nanorobots) may just be still too soon, but there are definitely some things I’d thought, or at least hoped, would have happened by now.
Joining Matthew Holt (@boltyboy) on #THCBGang on Thursday July 21 were futurist Ian Morrison (@seccurve); medical historian Mike Magee (@drmikemagee); and fierce patient activist Casey Quinlan (@MightyCasey)
You can see the video below & if you’d rather listen than watch, the audio is preserved as a weekly podcast available on our iTunes & Spotify channels.
I was at the AHIP conference in Vegas late last month and caught up with a number of CEOs & execs for some quick bite interviews — around 5 mins getting (I hope) to the gist of what they & their companies are up to. I am dribbling them out –Matthew Holt
I read the Stat News investigative piece “Health care’s high rollers,” by Bob Herman and colleagues, with interest but not much surprise. I mean, is anyone surprised anymore that healthcare CEOs often make a lot of money, and didn’t let a crisis like the pandemic dampen that? As Kaiser Family Foundation’s CEO Drew Altman told them, “Health care has become big business. We have a lot of people making a lot of money in health care, and we still have an affordability crisis in health care.”
I periodically see Twitter threads lamenting how little of that healthcare spending actually goes to physicians, yet people often still blame them for that spending. Physicians make a pretty decent living (an average of $322,000, according to the 2022 Medscape Physician Compensation report), although that compensation depends on specialty, gender, race/ethnicity, and location. But maybe, just maybe, the problem in healthcare is that we’re not paying physicians enough – not nearly enough.
I was at the AHIP conference in Vegas late last month and caught up with a number of CEOs & execs for some quick bite interviews — around 5 mins getting (I hope) to the gist of what they & their companies are up to. I am dribbling them out–Matthew Holt
It’s been a while but Anish Koka, a one time regular writer on THCB and occasional THCB Gang member, is back publishing up a storm on his Substack channel. You may recall that his political and clinical views don’t always mesh with some of the wooly liberals we feature on THCB (cough, cough, me), but we are delighted to be back publishing some of his pieces–starting with a look at a tweet from one of America’s most prominent cardiologists.–Matthew Holt
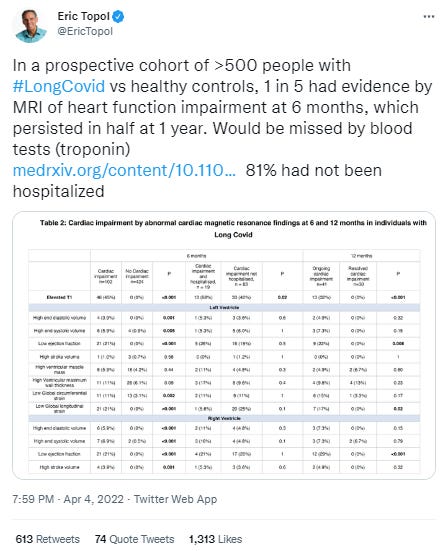
Given Twitter’s commitment to the truth in Medicine, I thought I would try to give them a hand by analyzing a semi-viral tweet about COVID and the heart.
Earlier this year (April 2022), the most influential cardiologist in the world tweeted about a study on the long term cardiac effects of COVID (LongCOVID).
Medical trainees who trained in the early 2000s like I did know Dr. Topol as an absolute legend in the field of Cardiology. He was responsible for seminal work in Cardiology in the 1980’s on the use of clot busting drugs for patients having heart attacks, and became head of cardiology for the famed Cleveland Clinic at the age of 36! (I vaguely recall feeling like I was starting to understand Cardiology at the age of 36.) He’s since moved on to do many other things, and is a potent voice that may have been instrumental in the FDA delaying approval of the mrna vaccines until after the 2020 election.
Nonetheless, this paper that he is giving his significant stamp of approval to has significant issues. As far as I can tell individuals with LongCOVID were recruited by advertising in LongCOVID support groups. No independent assessment carried out as far as I can tell clinically. If you say you have it—> you’re in.
I was at the AHIP conference in Vegas late last month and caught up with a number of CEOs & execs for some quick bite interviews — around 5 mins getting (I hope) to the gist of what they & their companies are up to. I am dribbling them out–Matthew Holt