Tom Kelly is the CEO of Heidi Health, another of the many ambient AI scribes that is spreading its wings to other roles, including bringing its own AI Open Evidence competitor! He calls it an AI care partner. Heidi started in Australia, and quickly moved to the UK and Canada, but now are in over one hundred countries. More recently they have come to the US and have now four major health systems and a lot of other mid market users. Tom think’s Heidi will soon do all the “work around the work”, and he doesn’t think it has to be deeply integrated with the EMR. He sees that as a superpower as doctors don’t want to be in the record. Is he right? Are scribes and ambient AI going to be separate? Does the scribe have to be a medical device, as it does in the UK? Will patients use it? Lots of questions about the future and Tom has lots of answers. Some might even be right!–Matthew Holt
Above the Fold
Dyslexia Comes Back To Bite President Trump

By MIKE MAGEE
This past week, Donald Trump decided to get into a war of words with a person with dyslexia. His target was the Governor of California, Gavin Newsom, who has struggled with the learning disability since the age of 5.
The President’s action was premeditated and intended to take the potential Democratic 2028 Presidential contender down a peg. It got pretty personal pretty fast. Trump was direct as is his way. He said simply, “Everything about him is dumb.”
In response, the governor broadened the conversation to include young Americans with the condition with these targeted words of encouragement, “To every kid with a learning disability: don’t let anyone — not even the President of the United States — bully you. Dyslexia isn’t a weakness. It’s your strength.”
Trump seemed surprised by the blowback from his “dumb” remark. It drew a stern rebuke from the Yale Center for Dyslexia and Creativity which reminded the President that approximately 20% of the US population is challenged by some form of this condition.
Fellow dyslectic, author and political commentator, Molly Jong-Fast, quickly connected the political dots to current events: “Mr. Trump is a bully, but beyond that he tries to flatten things. Sometimes voters respond to this flattening, this simplification of complicated issues, but ultimately his refusal to see nuance in things, his inability to plan ahead, to see second- or third-order effects is his undoing (see: this war he has gotten us into).”
As the Yale experts put it, “Reading is complex. It requires our brains to connect letters to sounds, put those sounds in the right order, and pull the words together into sentences and paragraphs we can read and comprehend. People with dyslexia have trouble matching the letters they see on the page with the sounds those letters and combinations of letters make. And when they have trouble with that step, all the other steps are harder.”
Neuroscientists couldn’t agree more. Language is indeed complicated. At least five areas have been identified as role players in coordinating human capacity for language and speech.
Continue reading…There Are Three Kinds of Primary Care, Not to Be Confused With Each Other

By HANS DUVEFELT
(Note: Hans is rerunning some of his greatest hits. This one is from 2014 and leans right into my current and future obsession with fixing primary care-Matthew Holt)
Primary care doctors, the way things are organized in this country, perform three kinds of services. If we don’t recognize very clearly just how fundamentally different they are, we risk becoming overwhelmed, burned out, inefficient and ineffective. And, if we think about it, should we really be the ones doing all three?
SICK CARE
Historically, people called the doctor when they were sick. That service has, at least in this country, become more or less viewed as a nuisance in primary care offices. We keep a few slots open for sick people, in part because the Patient Centered Medical Home recognition process requires us to. But our clinics may worry that those slots go unfilled and lead to lost revenue.
Instead, sick people scatter toward emergency rooms with crowding, high overhead and liability driven testing excesses or to freestanding walk-in clinics that only sometimes are integrated with the primary care office but universally staffed by providers who don’t know the patient. These providers, due to staffing cost strategies, are sometimes the least experienced clinicians within their organizations, doing what I feel is the most challenging work in health care – sorting the very sick from the only moderately ill or even completely healthy but worried patients.
In the worst case scenarios, the walk-in clinic is freestanding, operating without any access to primary care or hospital records, starting from absolute scratch with every patient. Some of these clinics are well equipped, with laboratory and x-ray facilities and highly skilled staff. But some are set up in a room in the back of a drug store and staffed by a lone nurse practitioner with minimal equipment and no backup.
Because health care in this country has no master plan, this is what has emerged. If we had a national strategy for health care services, does anybody think it would look like this?
CHRONIC DISEASE MANAGEMENT
More and more people suffer from chronic diseases like diabetes, hypertension and autoimmune conditions. This is where the bulk of primary care work is done. Much of it is straightforward and predictable: Diabetics get their glycosylated hemoglobin checked every three months, hypertensives get their blood pressure logs and blood tests reviewed at certain intervals. And, sadly, much of it is ineffective. Few people lose weight, improve their blood sugars or change their lifestyles. Our visits follow the same tired routine from one time to the next – “I’ll do better this time, Doc”.
The more our country’s chronic disease burden increases, the more clinician time and effort this kind of work will consume. And the more we need to question whether there isn’t a better way to deliver chronic disease management.
Continue reading…Oh. Another Moonshot

By KIM BELLARD
If all goes well, in the next couple of days NASA will be sending astronauts on their way to the moon, for the first time since – gulp – 1972. They’re not landing, mind you, they’re just doing a fly around, something Apollo 8 first did way back in 1968. Given the advances in microchips, computing power, AI, a robust private space industry, and Elon’s grand plans to inhabit Mars, it doesn’t really sound all that ambitious, hardly a “moonshot” in the sense that we’ve come to use that term, but I guess we should be glad that NASA hasn’t entirely conceded space to the billionaires.
The Artemis II mission will send four astronauts – including, if you are counting (and many are), the first person of color, the first woman, and the first Canadian to reach the moon — on a ten day, 230,000 mile trip that won’t actually orbit the moon but just loop around it, not getting closer than a few thousand miles. “Things are certainly starting to feel real,” Christina Koch, one of the four, said during a news conference Sunday morning.
Last week NASA unveiled its “Ignition” strategy that Artemis II is part of. It includes not just the fly-by, but also a follow-up mission in 2027, a manned landing in 2028, and a permanent moon base in the 2030’s, committing $20b over the next seven years to accomplish the latter. “NASA is committed to achieving the near‑impossible once again, to return to the Moon before the end of President Trump’s term, build a Moon base, establish an enduring presence, and do the other things needed to ensure American leadership in space,” said NASA Administrator Jared Isaacman.
He added: “Today, we are providing a demand for frequent crewed missions well beyond (previously announced moon landings in 2028). We intend to work with no fewer than two launch providers with the aim of crewed landings every six months, with additional opportunities for new entrants in the years ahead. America will never again give up the moon.”
I knew Elon and Jeff were going to get something from all this.
Continue reading…Today’s April Fool is me in 2011
I randomly found this interview I had completely forgotten about on Youtube from 2011. I was younger and thinner then, even though I didn’t have much hair. And I was very optimistic that tech was going to change health care in 10 years……and that it was going to take a long time. Guess we are still waiting!
Kevin Wang, Suki
Suki is one of the original Ambient scribing, now Ambient intelligence, companies. They’re selling both to providers and to other partners using their tech in their tools and services (think telehealth, other EHR providers like Athena, and more). Kevin Wang is the Chief Medical Officer, and he told me about the evolution of ambient documentation, how it makes doctors happy, and how it’s now moving into improving coding (and billing) but will soon be moving into improving clinical decision support. We haggled a little about the ROI from Ambient and where that comes from (remembering codes), and discussed how the EMR v Ambient plays out. And we talked a little about what the impact of ambient and AI will be on medicine…–Matthew Holt
Healthcare’s Quiet Dependence on the “Possimpible”

By GANESH ASAITHAMBI
In an episode of the sitcom How I Met Your Mother (HIMYM), Barney Stinson introduces a fictional word: possimpible. The possimpible combines “possible” and “impossible” and describes the extraordinary achievements by people who refuse to accept conventional limits. In modern healthcare, the possimpible is no longer a joke; it has quietly become an expectation.
Clinicians are expected to provide care that is safer, faster, and more compassionate despite rising administrative burdens, workforce shortages, and an increasingly complex patient population. These expectations often extend beyond what existing systems were designed to accommodate. The distance between what the system can provide and what patients need is increasingly filled by clinicians.
Picture this example at the end of a clinician’s day. A physician takes a seat to call a patient’s family. The phone conversation takes longer than expected with questions about their loved one’s prognosis and hesitancy about what to do next with fear about what is to come. The physician provides reassurance and guidance. The physician hangs up, only to find that note dictations are not complete and messages are still unread. None of this shows up as productivity, but it is needed to provide quality care. There are thousands of scenarios like this that take place every day in American health care.
These moments appear routine. However, they reflect something more consequential: healthcare has become quietly dependent on clinicians to stretch beyond the boundaries of the systems they work within.
Continue reading…Adventures in health care billing. My $51.96 zit co-insurance

By MATTHEW HOLT
I know my many fans love me delving into the world of why we get seemingly incorrect trivial bills in health care, and what they all mean. The long telenovella of the $39.94 bill from Labcorp is as yet stalled with One Medical apparently resubmitting the original claim with the new preventative codes on it. But even though I am continuing and expanding my role as a difficult patient this year, there are still some blasts from the past that won’t quite leave.
This particular one concerns some rather unpleasant dermatology issues. For many years I had an nasty small sore/lesion on my leg that never quite healed. Then I started getting a few more that started as zits and never quite left. My wise PCP Andrew Diamond at One Medical told me to use some antibiotic wash and referred me to a dermatologist. Unfortunately the one I was referred to was out of network for the Blue Shield HMO I was in, but one request back to One Medical and I was both sent to a dermatologist in my network and got a pre-auth in the mail from Blue Shield to go see him!
Dr Cristian Gonzalez took a quick look at my leg, decided what the problem was, and proceeded to inject, freeze and attack my various lesions. He then prescribed a cheap topical steroid for me to use, and basically after 4 visits over the summer and Fall, my legs went back to resembling a baby’s bottom–well more or less.
For each specialty visit Blue Shield had a co-pay of $85 per visit, which I handed over using my HSA card. One time the front desk said I had a balance, but when I asked them what it was for they told me it was a mistake. Until this week.
Some 4 months after my last visit I got a bill in the mail for $51.96
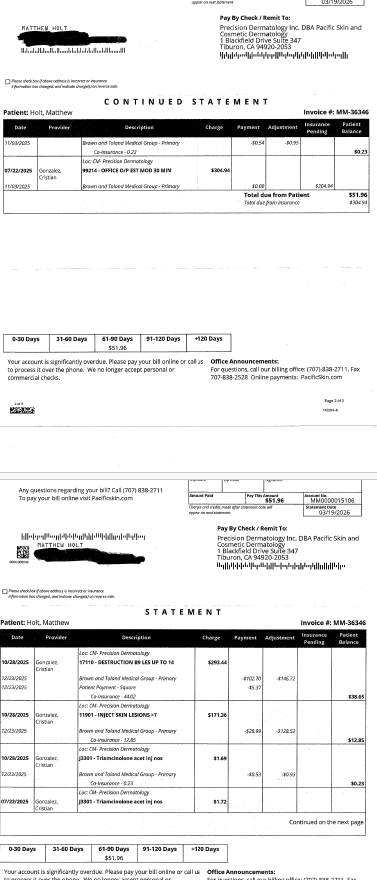
Given that I had made a co-pay of $85 each time, this seemed a little odd. So I took a look at my Blue Shield EOBs. (BTW they are back online, you may recall they vanished when Blue Shield cancelled and then changed my plan but the Internet never forgets….)
There a curious anomaly began to play out. Each visit generated three identical claims and three more or less identical EOBs.
Continue reading…Calling BS
By KIM BELLARD
We are living, you’d have to say, in the age of bullshit. Our politicians can’t answer the simplest of questions without spouting word salad answers aimed at running out the clock until the next question. Our corporations spew endless platitudes about their lofty goals in an attempt to distract us from their mendacious profit-seeking. And now we have AI producing endless volumes of words, an unpredictable amount of which aren’t remotely true.
For better or worse (and, trust me, it has often been for worse), I’ve always been one to ask “why,” to probe vagueness — whether it was a teacher, a boss, or a politician. Call me cynical, call me skeptical, call me inquisitive, but I have a low tolerance for bullshit, in its many forms. So I was thrilled to see that a new study suggests that employees who don’t fall for corporate bullshit may be better employees.
The study is from Shane Littrell, a postdoctoral researcher and cognitive psychologist at Cornell University, whose research “focuses primarily on how people evaluate and share knowledge, particularly the ways that misleading information (e.g., bullshit, conspiracy theories, corporate messaging) influence people’s beliefs, attitudes, and decisions.”
One wonders what he was like as a child.
His new research introduces a new tool called the Corporate Bullshit Receptivity Scale (CBSR), which was “designed to measure susceptibility to impressive-but-empty organizational rhetoric.”
His paper defines “bullshit” as “a type of semantically, logically, or epistemically dubious information that is misleadingly impressive, important, informative, or otherwise engaging,” and distinguishes it from other types of speech (such as jargon) in that “it is both functionally misleading and epistemically irresponsible.”
Continue reading…Ian Shakil, Commure
Ian Shakil is the Chief Strategy Officer of Commure, the AI platform being used by HCA, Tenet and others. He came to Commure via its acquisition of Ambient AI vendor Augmedix, and there are a lot other other new acquisitions within Commure (Athelas, PatientKeeper, Memora Health, Rx Health etc). We dived in not only about what Commure does but the big question of how does a client like HCA or Tenet decide what Commure does, vs what Meditech does, vs what Google does vs what they do internally. We also (sorta) looked into the various criticisms (basically all from Sergei Polevikov!) of what Commure and its main funder General Catalyst are up to and what is happening at Summa Health the hospital in Ohio that GC bought. He also says the good experience from AI will come to help patients this year, and I’ll be holding him to that!–Matthew Holt







