On the morning of November 9th, the day after the 2016 U.S. Presidential Election, a visceral sense of shock was felt throughout the campus of Harvard Medical School. Donald Trump’s victory appeared to be an abrupt rebuke of so many of our commonly held values—equality, service, compassion. As medical students and physicians in Boston, we understood that we were isolated—both geographically and ideologically—from the myriad forces that swept Mr. Trump into office. However, there was something unsettling about our collective disbelief. How was it that so many of us had failed to recognize the depth of pain and divisiveness that existed within our country? There arose, in all of us, a need to understand.
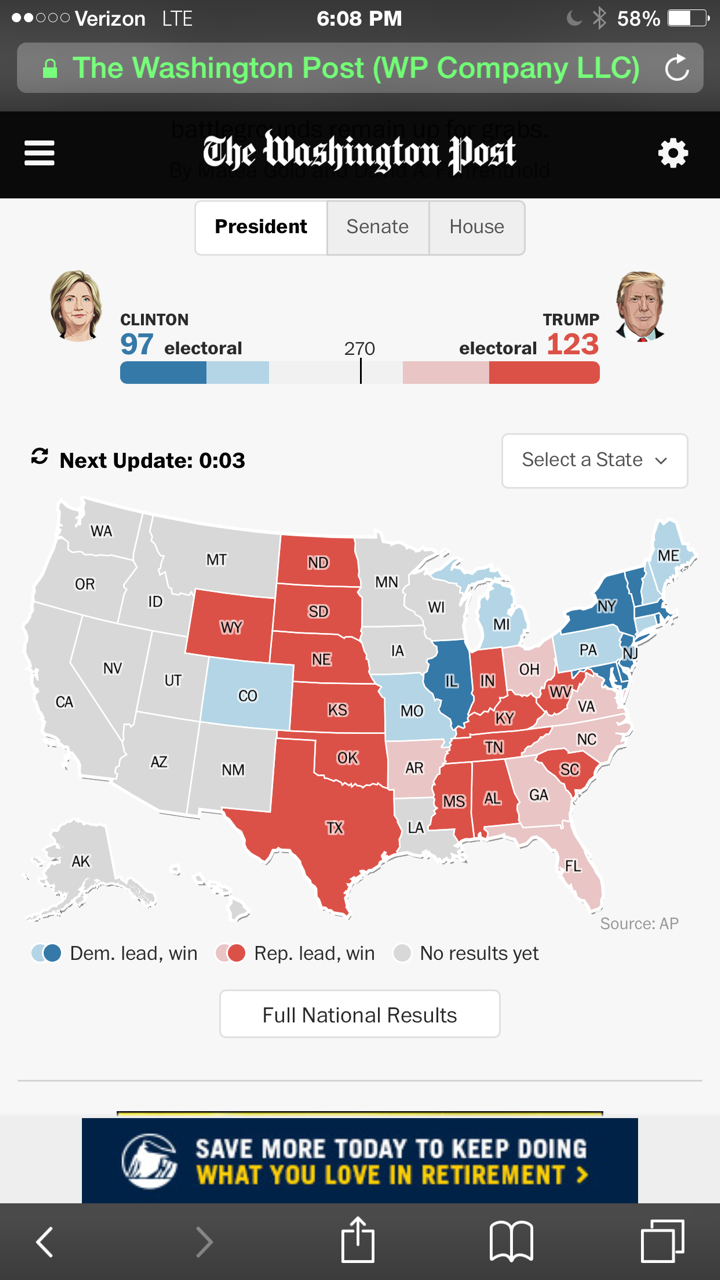
In the aftermath of the election, political analysts have ascribed Trump’s victory to several themes—condemnation of the intellectual elite, widespread economic disaffection, and the rise of a potent strain of populism. However, closer inspection reveals another contributor to this startling election result. Though the final votes are still being tallied, it is clear that Mr. Trump will have received fewer votes in victory than the previous two republican nominees garnered in defeat. Instead of representing a powerful mandate, Mr. Trump’s victory hinged on vast portions of the electorate choosing to stay home. Nearly half of all Americans did not cast a ballot in this election1. As captured poignantly by Jon Favreau, former speechwriter to President Obama, “democracy is fragile and belongs to those who show up.” Continue reading…



 What if your spouse were a borderline Type 2 diabetic? If you had the money, you could hire someone to follow her or him around the clock, sort of like a glorified personal trainer. Your spouse would make sure he or she took a daily mile-long walk, did some weight training to build muscle mass and would stop you from eating ice cream or cake or drinking a glass of wine.
What if your spouse were a borderline Type 2 diabetic? If you had the money, you could hire someone to follow her or him around the clock, sort of like a glorified personal trainer. Your spouse would make sure he or she took a daily mile-long walk, did some weight training to build muscle mass and would stop you from eating ice cream or cake or drinking a glass of wine.









