 Patients with End Stage Renal Disease (ESRD) constitute a high-cost, high-need population that can greatly benefit from targeted policy initiatives to improve care coordination. In 2010, patients with ESRD made up 1.3% of the Medicare population, but accounted for 7.5% of total Medicare spending, amounting to over $20 billion.1 Adoption of the accountable care organization (ACO) model for ESRD has the potential to improve care coordination and patient outcomes. Due to complex health needs, patients in this population can require visits to multiple providers with multiple care plans. By bringing these providers together under the same organizational structure, accountable care provides the opportunity to improve quality through coordination. Though just over 1 million ESRD beneficiaries participated in the Pioneer ACO program, to date no direct studies have examined the effect of ACOs on management of ESRD.
Patients with End Stage Renal Disease (ESRD) constitute a high-cost, high-need population that can greatly benefit from targeted policy initiatives to improve care coordination. In 2010, patients with ESRD made up 1.3% of the Medicare population, but accounted for 7.5% of total Medicare spending, amounting to over $20 billion.1 Adoption of the accountable care organization (ACO) model for ESRD has the potential to improve care coordination and patient outcomes. Due to complex health needs, patients in this population can require visits to multiple providers with multiple care plans. By bringing these providers together under the same organizational structure, accountable care provides the opportunity to improve quality through coordination. Though just over 1 million ESRD beneficiaries participated in the Pioneer ACO program, to date no direct studies have examined the effect of ACOs on management of ESRD.
The Centers for Medicare and Medicaid Services (CMS) recently announced the participants in the Comprehensive ESRD Care (CEC) Model.2 This program will create ESRD Seamless Care Organizations (ESCOs) to promote care coordination across settings for dialysis patients. We created groups of potential ESCO participants based on provider ownership and locations announced by CMS. We examined quality data available from the Dialysis Compare database for these potential participant organizations and learned that collectively they have a quality score slightly lower than the national average, and there is considerable variation in quality by geographical location and ownership. While CMS has been progressive in its initiatives to improve quality and lower costs for this complex patient population, our analysis indicates that ESCOs have room to improve ESRD patient care over their baseline performance. Because ESCOs can realign patients from existing ACOs, it is important to understand the potential effectiveness of ESCOs and the ramifications for the health system as a whole.
Medicare Payment for ESRD Services
In 1972, the Medicare ESRD program was enacted as the only disease-specific entitlement program within CMS. Medicare Part A and B benefits were extended to include any individuals with ESRD (of any age) entitled to receive social security benefits. Changes to reimbursement for dialysis care continued through the 1980s and 1990s, including the establishment of a bundled payment for routine dialysis care and changes in prescription billing. More recently, CMS implemented two important programs to reduce costs and improve quality for this population: the ESRD Prospective Payment System (PPS) and the ESRD Quality Incentive Program (QIP).3,4 Through these programs, prospective payments are given to dialysis facilities and include all billable items related to a single dialysis session. The QIP introduced performance measurements alongside the PPS by penalizing dialysis facilities for failing to meet anemia and dialysis quality targets. Combined, these initiatives resemble ACOs with the dual focus of cost reduction and quality improvement. In contrast to the ACO model that attempts to achieve these goals through improved care coordination between inpatient and outpatient settings, the current ESRD model does not include coverage across the continuum of care. In 2013, CMS announced the CEC Model concept to adapt care coordination principles from the ACO Model to the ESRD population, and in October 2015 announced the participating ESCOs.
Overview of the Comprehensive ESRD Care Model
The CEC Model targets this patient population, characterized by multiple comorbidities and polypharmacy, with the goal of improving care processes, clinical outcomes, beneficiary experiences of care, management of care transitions, as well as reducing utilization and costs. It does so by establishing ESCOs, organizations that receive shared savings payments through the CEC Model to encourage lower costs and improved quality of care. If successful, this disease-specific accountable care model could provide the blueprint for other groups of patients with unique and complex medical conditions. Given the historical background of CMS’ relatively active role in managing costs and quality for this patient population through the PPS and QIP, one question is how much potential for improvement participating organizations have under the ESCO model.
On October 7, 2015, CMS announced the 13 ESCOs participating in the CEC Model. These include 12 “large dialysis organizations (LDOs)” (one owner with more than 200 dialysis facilities) and one non-LDO (fewer than 200 facilities). The list of ESCOs includes information on the organization’s name, the participating dialysis provider organization (owner), and the city and state in which the ESCO is located. Using this information, we drew upon available performance data from CMS’ Dialysis Compare database to examine previous performance of potentially attributed dialysis facilities. While this methodology is not exact, given the information provided, it offers a method for examining regional providers under the same ownership to inform likelihood of ESCO success. We were unable to match information for one organization, Liberty Kidney Care Alliance, LLC. Our analysis contains 11 LDOs and one non-LDO matched to 169 identified dialysis facilities. To compare facilities on quality performance, we utilized the Dialysis Compare five star rating system and total performance score for payment year 2015.5,6
Baseline Performance of ESCO Participants
CMS utilizes the five star quality rating system as a metric for patients to understand the relative quality of individual dialysis facilities, with 3 stars representing an “average” score. The five star measure is a composite of 3 years of performance data from 2011–2014 and compares individual facilities reporting to Dialysis Compare, relative to one another, with each star level representing a performance quintile. A facility can have poor quality, but if its quality is superior to other facilities, that will be reflected in a higher star rating. The majority of dialysis facilities included in the ESRD CEC Model have average five star quality scores (46%). 30% of dialysis facilities are below average (two stars or less) and 23% are above average (four or five stars). The average five star rating for potential ESCO participants is 2.9 (below average). The majority of included facilities are for-profit (90%) and owned by a dialysis chain (96%). Additionally, CMS scores participating dialysis facilities on a 1 to 100 scale through the QIP. This total performance score is a composite measure of a facility’s performance on quality measures. It is an objective quality performance score, in contrast to the relative comparison score provided by the five star rating. The average performance score of potential ESCO participants is 79.6, just below the national average of 81. For our analyses, we aggregate the measures of these individual facilities at the ESCO level.
Figure 1. Estimated ESCO Participant Star Ratings 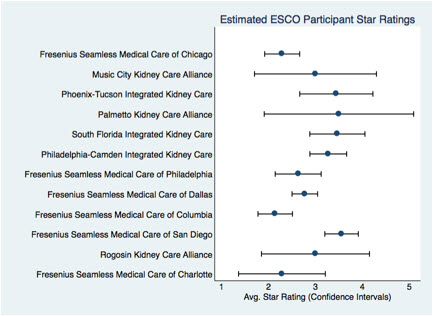
Figure 2. Estimated ESCO Participant Performance Score
Room for Improvement
As the graphs indicate, while some estimated ESCO participants perform higher on the quality scale than others, every participant has some room for improvement. Many potential participants vary widely in the range of quality performance amongst individual facilities contained within the ESCO (Figure 2). Using current data, the upper bounds of the confidence intervals of three participants did not reach the national average in quality performance, and the mean quality performance score fell below the national average for six potential participants. Conversely, five potential participants have average quality scores above the national average. While CMS has been progressive in adoption of quality improvement and payment reform for the ESRD population through the QIP and PPS, improved coordination of care can further improve patient outcomes in the initial cohort of estimated ESCO participants. The baseline variation of potential ESCO participants will also provide important insights as to what types of organizations will prove successful as ESCOs. Future research should examine performance variation within ESCOs to determine impact on eventual outcomes.
Beneficiary Alignment
More broadly, 91% of Medicare beneficiaries with ESRD are not currently aligned to Medicare ACOs.7 In the states of participating ESCOs, only 8.7% of beneficiaries are presently aligned to Medicare ACOs. ESCOs therefore have ample opportunity to coordinate care for patients not currently receiving improved care coordination through a Medicare ACO. By reducing costs and improving quality for these high-cost, complex ESRD patients, ACOs and ESCOs have the opportunity to translate optimal performance into shared savings payments.
Notably, the interplay between ESCO and ACO patient attribution will be important to monitor. Attribution of ESRD patients to ESCOs has the potential to draw from existing ACOs’ rosters of high-cost, high-need patients, impacting the likelihood of achieving shared savings for those ACOs, and therefore their viability of long-term success. If a beneficiary is already assigned to a Pioneer ACO, Next Generation ACO, or Medicare Shared Savings Program (MSSP) Track 3 ACO (highest risk sharing), the beneficiary will remain aligned with that ACO. However, if a beneficiary is prospectively aligned with a Track 1 or Track 2 MSSP, that beneficiary will be eligible to be permanently assigned to an ESCO. This potential realignment could represent revenue loss for Track 1 and 2 MSSPs, yet improved outcomes for ESRD patients. It will be important to measure the success of ESCOs in achieving the goals of cost reduction and quality improvement, as well as the unintended consequences that may impact performance in nearby Track 1 and 2 MSSPs. While our analysis has demonstrated ESCOs’ potential, their success must be monitored in the context of Medicare’s system-wide transition to value-based payment.
Endnotes/Citations
1. Centers for Medicare & Medicaid Services. Comprehensive ESRD Care Model Fact Sheet. 2014; https://www.cms.gov/Newsroom/MediaReleaseDatabase/Fact-sheets/2014-Fact-sheets-items/2014-04-15.html.
2. Centers for Medicare & Medicaid Services. Comprehensive ESRD Care Model. 2015; https://innovation.cms.gov/initiatives/comprehensive-esrd-care/.
3. Centers for Medicare & Medicaid Services. ESRD Prospective Payment System (PPS) Overview. https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/ESRDpayment/.
4. Centers for Medicare & Medicaid Services. ESRD Quality Incentive Program. https://www.cms.gov/medicare/quality-initiatives-patient-assessment-instruments/esrdqip/index.html.
5. Centers for Medicare & Medicaid Services. Dialysis Facility Compare datasets. https://data.medicare.gov/data/dialysis-facility-compare.
6. Centers for Medicare & Medicaid Services. Dialysis Facility Compare Total Performance Scores (PY 2015). https://www.medicare.gov/dialysisfacilitycompare/ – qip/total-performance-scores.
7. Centers for Medicare & Medicaid Services. Total number of Medicare FFS beneficiaries with ESRD not aligned to Medicare ACOs by State. https://innovation.cms.gov/Files/x/ACO_FFS_statealignment.pdf.
Categories: Uncategorized







