As Barack Obama’s presidency draws to a close, we anticipate growing discussion of his legacy. Much of that discussion will focus on the Affordable Care Act (ACA), his signature legislative accomplishment. The legislation is complex and in some cases ineffective and cumbersome. It can be argued, for example, that the complexity of the ACA favors the same high-cost, legacy health care players that the bill was designed to address.
But one of the major goals of the ACA was to provide more accessible, more dignified, and more effective health care to the poor. And in this respect, we believe that the Affordable Care Act – at least in those states that have elected to expand Medicaid – has been a success.
Our perspective on health care reform comes from ACAView, a joint initiative between the Robert Wood Johnson Foundation (RWJF) and athenahealth to study the impact of health care reform. We have just released our latest report, The Effects of the Affordable Care Act through 2015, which focuses on the impacts of insurance coverage expansion for patients and providers, with an emphasis on primary care. This report analyzes data from 21,900 health care providers on athenahealth’s network for at least five years. These physicians, who serve communities across the nation, are broadly representative of the country as a whole (please refer to the Appendix of the latest report). This allows us to compare physician practice before and after the coverage expansion provisions went into effect in 2014.
In June 2012, the Supreme Court ruled in “National Federation of Independent Business (NFIB) v. Sebelius” that states could choose whether or not to expand Medicaid eligibility. Although the federal government would cover the full cost of coverage expansion through 2016 and gradually decreasing to 90 percent of it thereafter, about half of the states declined to provide expanded Medicaid access to low income people. Since that time, six of those states have changed course and made Medicaid available to more of their residents.
In those states that agreed to loosen Medicaid eligibility requirements, there was no guarantee that the law would improve health care access for low income people. Because Medicaid payment levels are much lower than commercial rates, some observers were concerned that physicians would not open their schedules to see more Medicaid patients. And when patients did come in for care, no one knew whether they would form ongoing relationships with physicians or merely receive one-off care for acute or symptomatic issues.
Within the athenahealth network, several observations are clear:
- Most physicians are seeing more Medicaid patients
- New Medicaid patients, especially those with chronic conditions, are establishing ongoing relationships with primary care physicians; and
- Physicians are spending just as much time with Medicaid patients as they are with commercially insured patients.
The impact of expanded Medicaid coverage on primary care physicians’ (PCPs) practices occurred rapidly. Prior to 2014, PCPs in Medicaid expansion states using athenahealth services saw a Medicaid case-mix – the share of visits from Medicaid patients – of 15 to 16 percent. Within nine months after the coverage expansion provisions of the ACA went into effect, this proportion had increased to 21 percent as doctors increasingly accepted new Medicaid patients. The primary care physicians in our sample saw an average of 33 percent more Medicaid patients in 2014 than in 2013. Over the life of athenahealth, we have not seen a change in physician payer mix that even approaches this magnitude.
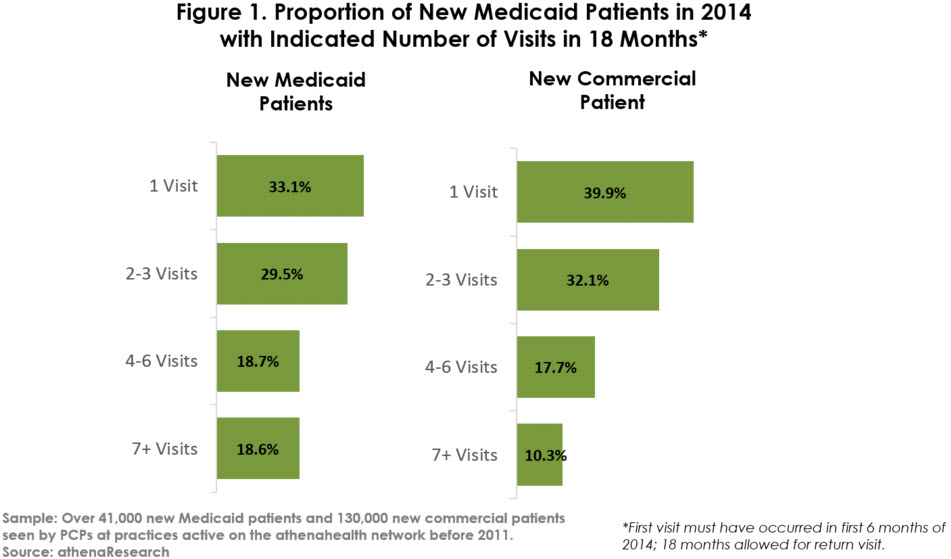
Rather than receiving one-off, episodic care, these new Medicaid patients are establishing new relationships with primary care physicians. As shown in Figure 1 below, 67 percent of new Medicaid patients in the first six months of 2014 returned for a second visit. In fact, more than 37 percent returned for four or more visits by the end of 2015. Their return rate was actually somewhat higher than that of commercially insured patients, who were more likely to receive only one visit and less likely to receive four or more visits.
Moreover, patients with greater health needs are more likely to return for ongoing care. We measured the return rates for patients with four chronic conditions: diabetes, hyperlipidemia, hypertension, and mental illness.1 As shown in Figure 2, patients with more chronic conditions returned at higher rates. For example, 72 percent of patients with one to two chronic conditions returned for a second visit, as did 82 percent of patients with three to four of the selected chronic conditions. Similar rates of return were observed for new commercially insured patients, suggesting that PCPs are providing Medicaid patients with good access to care.

Not only are primary care providers willing to take on more Medicaid patients, but they also appear to be spending the same amount of time with their Medicaid patients as with their commercial patients. We estimated visit times based on the time providers spent actively recording and documenting the visit in our athenaClinicals EHR while they were with patients. (Although there are limitations inherent in estimating visit time from software utilization patterns, the same methodology is used across all visits. We therefore consider this methodology valid for comparing visit time differences in different patient and provider cohorts.) From 2013 to 2015, average visit times for patients with Medicaid coverage were essentially the same as for commercial coverage, although visits with uninsured patients were slightly shorter.
One of the goals of the ACA was to ensure that more low-income people take advantage of Medicaid coverage to establish stable relationships with primary care physicians. At least for patients seeing primary care physicians in expansion states, this aspect of Obamacare is working. Moving forward, we will be taking a closer look at this cohort of newly insured patients to determine whether patient outcomes are improving in the states that chose to expand Medicaid eligibility.
As always, we welcome input and suggestions for future work.
1Patients were categorized based on the number of selected chronic conditions that had been addressed (as measured by the diagnosis code on the claim) during their first visit.
Josh leads the athenaResearch team’s efforts in mining athenahealth network data for insights into physician performance and the US health care system.
Categories: Uncategorized







