According to the latest count, there are 255 Health Information Exchange (HIE) organizations across the country, which amounts to an average of 5 in each State. If you are a practicing physician and have an EHR, chances are someone already knocked on your door offering to connect your practice to the local HIE for a small fee. If you don’t have an EHR, you may have had offers to access an HIE web portal, or maybe an HIE supplied EHR Lite, allowing you to at the very least view clinical data from other sources. Perhaps for free. If you are the proud owner of one of the full-featured EHRs, you may wonder what an HIE can do for you that your EHR is not already doing, and whether that service is worth your hard earned money.

In theory, a top-shelf EHR should be able to connect your practice to multiple facilities and allow you to exchange information to the best of all participants’ abilities. Granted most EHRs are still working on some of the connections, particularly to local facilities, but all in all, an EHR should be able to eventually provide for all your connectivity needs as shown in Figure 1. Note that for some types of connections, your EHR vendor can use a clearinghouse or portal approach to simplify and reduce costs of connectivity. For example, you don’t need a separate interface for each pharmacy – you use Surescripts as the clearinghouse and let them worry about it. You also don’t need an individual connection to each patient’s home – you communicate with all of them through one portal. With the exception of Surescripts pharmacy connectivity and a small number of reference labs, each connection, or interface, is costing you a pretty penny, and the more local the connection, the longer it takes to build.
Enter the local HIE. The value proposition of a regional exchange is in connecting you to local hospitals, imaging centers, State agencies and community resources. Figure 2 shows a typical HIE arrangement.

If you compare this to Figure 1, it becomes apparent that your EHR vendor has a much easier job now. Instead of building an interface to each hospital, the vendor needs just one interface to the HIE and presto, you are connected to all hospitals. Yes, this is an outlandish oversimplification of affairs, since most players have no ability to connect to HIEs and since each message type requires its own separate interface (or special code to sort messages out). If your EHR vendor has a critical mass of customers in your area, all needing to connect to the same regional facilities, a connection to the HIE should create significant savings for the EHR vendor, and hopefully some of those savings will be passed down to you. The HIE will in turn try to get a portion of that money from you to cover their costs of building and maintaining interfaces. If there is more than one HIE in your referral region, your EHR vendor may need to repeat the effort for each HIE. This will increase the complexity and costs for all involved.
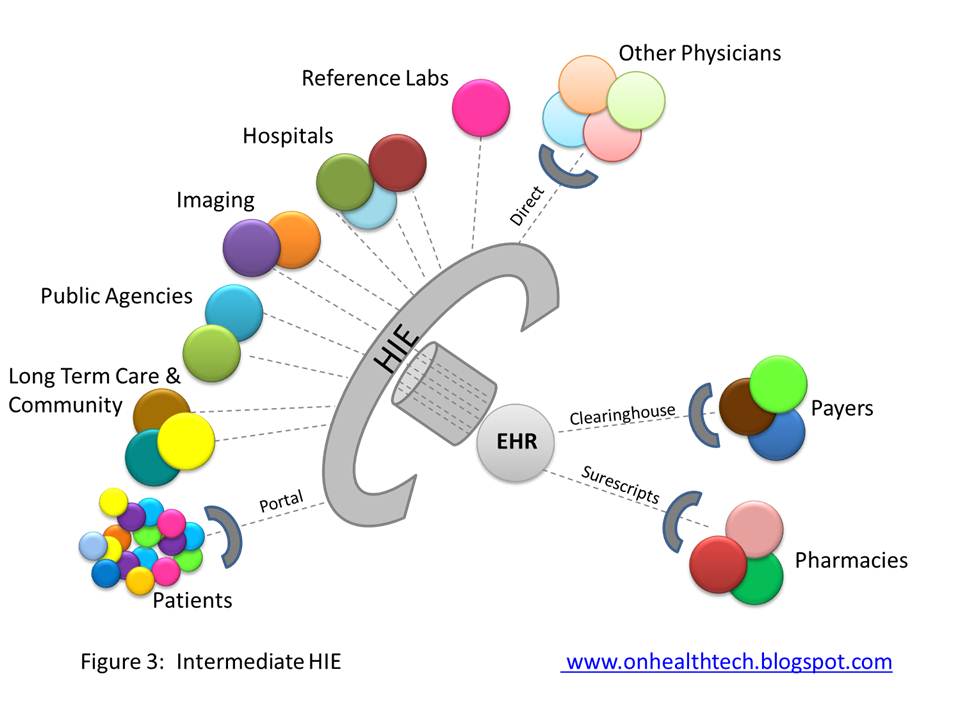
Some HIEs are trying to do more. Although EHR vendors are increasingly integrating abilities to exchange information between physicians through theDirect Project protocol, HIEs are attempting to do the same thing. Depending on your EHR vendor, the HIE may be a few steps ahead and will offer you that functionality. Of course, it will not be integrated in your EHR workflow, but it may still be worthwhile. Since most HIEs retain data exchanged through them (or have the ability to retrieve it from the source), they are also considering offering patients access to their data. If your EHR vendor does not offer a Patient Portal or charges a lot for one, this may be a very tempting proposition. Figure 3 illustrates this more comprehensive setup, which also includes connectivity to reference labs, as this is a simple thing to do and several HIEs are doing just that. The HIE menu of services in Figure 3 will cost you substantial subscription fees, and rarely some transactional fees, on top of what you are paying for your EHR.
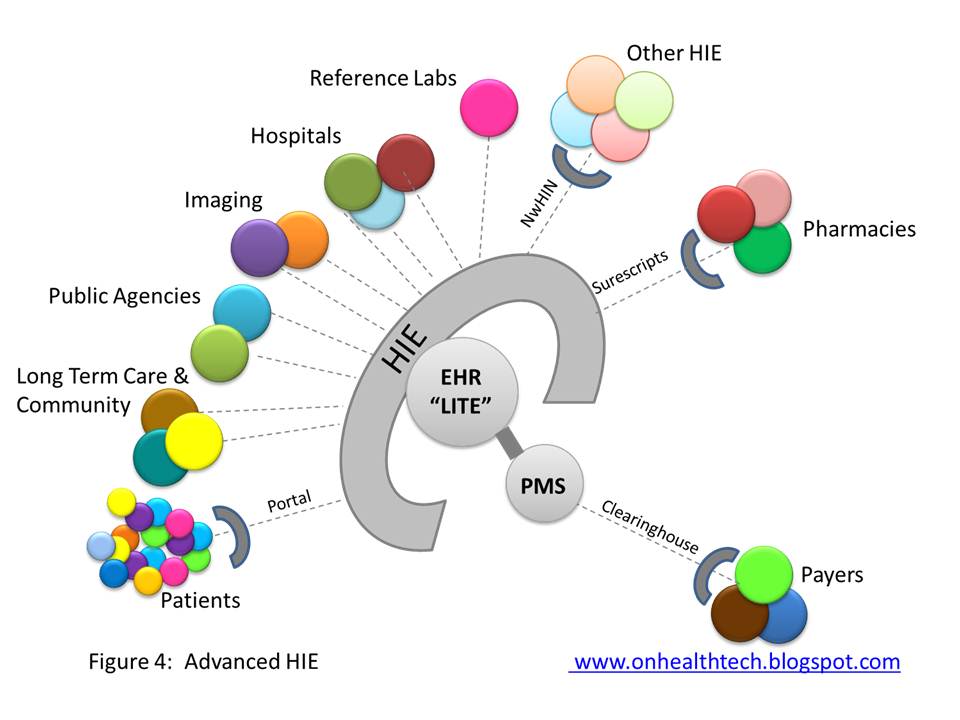
If you don’t have an EHR, some HIEs will offer you a one stop shop, which can include a lighter version of an EHR (geared to Meaningful Use), which includes electronic prescribing. This may be a cumbersome solution if you still need to maintain a paper chart, and perhaps this is why the top HIE vendors offer EHRs that are fully functional and which only need to be connected to your Practice Management System (PMS), as shown in Figure 4. In this scenario, you would have to pay the HIE a hefty price, but you won’t have to pay extra for another EHR. Finally, there is at least one HIE out there, and I am certain more will follow, which can accommodate your billing needs as well.

Having come full circle, Figure 5 illustrates the complete transformation of the HIE into a complete EHR and PMS. The difference between Figure 1 and Figure 5 is not just terminology. The system in Figure 1 stores data either in individual physician databases or in a national database of all EHR customers for an Internet based EHR. In Figure 5, you are accessing an EHR that contains the data of other physicians, hospitals and care agencies in your area. This is a much more powerful configuration and better suited to care coordination and care management. This is pretty much how large health care systems are set up and in most cases the HIE is run by their enterprise EHR vendor. In fact, just like HIE vendors are building EHRs, most large EHR vendors either have, or are quickly assembling, formal HIE capabilities (master patient index, good interface engine, robust database structures).
So here is a wild prediction: it may take a while, but eventually small EHR vendors will be replaced by strong HIEs, and weak, failing or nonexistent HIEs will be displaced by large EHR vendors who had the ability and wisdom to become HIEs, and there will be no distinction between the two types of software vendors. Right now the 255 HIE organizations across the country are struggling to find a way to become sustainable businesses, and most EHR vendors, while posting record profits, are struggling to provide much needed interoperability. A marriage of necessity is inevitable. What should we name the baby?
Margalit Gur-Arie was COO at GenesysMD (Purkinje), an HIT company focusing on web based EHR/PMS and billing services for physicians. Prior to GenesysMD, Margalit was Director of Product Management at Essence/Purkinje and HIT Consultant for SSM Healthcare, a large non-profit hospital organization. She shares her thoughts about HIT topics and issues at her blog, On Healthcare Technology.
Categories: Uncategorized







